First Chinese Human Gastric Peroral Endoscopic Myotomy for Diabetic Gastroparesis
- 1. Department of Gastroenterology, The First Affiliated Hospital of Soochow University, China
Abstract
Diabetic gastroparesis is a chronic functional syndrome caused by diabetes mellitus. Diagnosis is based on symptoms and scintigraphy. The therapeutic options are still limited. A publication has recently described the effectiveness of gastric per oral endoscopic myotomy. We herein present a case of diabetic gastroparesis treated by gastric peroral endoscopic myotomy which extended the submucosal tunnel on the front gastric antral wall instead of the posterior wall.
Keywords
• Diabetic gastroparesis
• Delayed gastric emptying
• Gastric peroral endoscopic myotomy
• Treatment
Citation
Zhang X, Shi D, Zhang D, Li R, Chen W (2016) First Chinese Human Gastric Peroral Endoscopic Myotomy for Diabetic Gastroparesis. JSM Gen Surg Cases Images 1(1): 1005
ABBREVIATIONS
DGP: Diabetic Gastroparesis; GCSI: Gastroparesis Cardinal Symptom Index; G-POEM: Gastric Peroral Endoscopic Myotomy; GI: Gastrointestinal Imaging; DGIM: Disorders of Gastrointestinal Motility; FDA: Food and Drug Administration; POEM: Peroral Endoscopic Myotomy
INTRODUCTION
Diabetic gastroparesis is a chronic complication of diabetes characterized by symptoms of gastric motility deficiency. The delayed gastric emptying caused by gastrointestinal movement dysfunction can significantly affect digestion and absorption of food, at the same time, due to the influence of absorption of oral drugs; it can also interfere with the treatment of diabetes. There is currently no effective treatment of the diabetic gastroparesis, this article reporting a case of treating the diabetic gastroparesis by gastric per oral endoscopic myotomy is in the hope of granting some hints to help clinical management
CASE PRESENTATION
A 27-year-old man was diagnosed with insulin-dependent diabetes mellitus for six years and had daily symptoms of nauseaearly satiety bloating, abdominal pain and vomiting one year ago. These symptoms led to his poor blood sugar control, therefore he was repeatedly admitted to the hospital because of ketoacidosis. His Gastroparesis Cardinal Symptom Index (GCSI) was 42. Upper gastrointestinal imaging (Figure 1)

Figure 1 Upper gastrointestinal imaging.
showed severely delayed gastric emptying, and gastroscopy showed visual reduction of gastric peristaltic wave. At the time of our evaluation, he was symptomatic despite a regimen consisting of domperidone, esomeprazole, and metoclopramide. Gastric peroral endoscopic myotomy (G-POEM) was then considered after he refused surgical interventions including pyloroplasty and subtotal gastrectomy considering the cost, risk of surgery and postoperative quality of life. This experimental procedure was discussed with the patient, who signed informed consent for the procedure.
The patient underwent this operation under the general anesthesia. After creating a submucosal bleb by injecting saline solution and 0.25% indigo carmine solution on the gastric antrum front wall 5 cm proximal to the pylorus, a submucosal tunnel to the pylorus was extended by using Hybrid Knife (Figure 2).
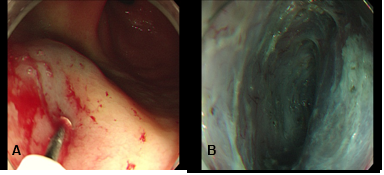
Figure 2 G-POEM for DGP: (A) – A mucosal incision was made 5 cm to the pylorus. (B) – Submucosal tunnel was extended by using Hybrid Knife. (C) – The circular muscle bundles were cut. (D) – Larger vessels in the submucosa were coagulated to insure there is satisfactory hemostasis. (E) – The mucosal entry was closed by endoscopic clips.
Subsequently, the circular muscle bundles was separated and cut with spray coagulation current. Care was taken to ensure that the larger vasculature were unimpaired. Coagulating the bleeding incision, and followed by closing the mucosal with 8 metal clips.
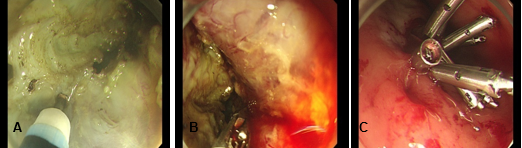
Figure 3 (A) – The circular muscle bundles were cut. (B) – Larger vessels in the submucosa were coagulated to insure there is satisfactory hemostasis. (C) – The mucosal entry was closed by endoscopic clips.
An upper GI series (Figure 4)
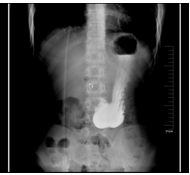
Figure 4 Postoperative barium meal followed the operation in case of leakage.
was obtained the following day and showed no evidence of leakage after postoperative fasting An upper GI series (Figure 4) was obtained the following day and showed no evidence of leakage after postoperative fasting for one week. The patient started a liquid diet and then a soft diet the following day. As showed an increased ability to tolerate frequent meals, he was discharged home. Postoperative barium meal (Figure 5)

Figure 5 Upper gastrointestinal imaging obtained 1 month latter.
performed 1 months postoperatively showed no evidence of gastric retention. By 3 months postoperative, the patient tolerated a regular diet and was nearly symptom free and the self-assessed GCSI had decreased to a total score of 6.
DISCUSSION
The concept of diabetic gastroparesis (DGP) was promoted by Kassander in 1958 at the first time [1], and then it was classified as disorders of gastrointestinal motility (DGIM) [2]. AS a well established complication of diabetes, the quantity of patients with DGP appears to be increasing as the rising of morbidity of diabetes.In a study by Choung RS et al in 2012, it is estimated that 50%-76% of diabetic population experience symptoms associated with delayed gastric emptying[3]. So far, however, the treatment of diabetic gastroparesis is still limited, and there is no unified standard in therapy and evaluation of curative effect. Metoclopramide is the only US FDA-approved medication for the treatment of gastroparesis for no longer than a 12-week period [4]. However, most patients experienced recurrent symptoms after they withdrawal of the treatment due to the side effects of these drugs [5]. For most patients with severe symptoms, it cannot achieve the purpose of controlling the symptoms with drug therapy alone [6]. Endoscopic intrapyloric botulinum toxin injection used to be a commonly treatment, however, its efficacy has still been highly controversial. A recent study reported that there is no significant benefit of endoscopic injection of botulinum toxin over placebo in improving either symptoms or rate of gastric emptying[7-8]. So, the American Gastroenterological Association currently does not recommend the use of this treatment for patients with gastroparesis [9].
A recently published study reported that laparoscopic pyloroplasty provided significant symptom reduction and accelerated gastric emptying scintigraphy in patients with DGP [10]. Jillian L. Angelo et al reported two 2 cases treated by pyloroplasty successfully [11]. However high-surgical-risk, postoperative complications and high cost of surgery restricted the popularity of this method. With the development and popularity of endoscopic technic, it is widely accepted that POEM is an effective method in patients with achalasia of cardia. It is opening up a new way in treatment of DGP, although the history of POEM is very short. We theorize that a subset of patients with refractory gastroparesis may respond to endoscopic pyloromyotomy by evaluating pyloroplasty and POEM. Kawai et al previously performed endoscopic pyloromyotomy in 8 pigs [12]. Then with the similar techniques, principles, and equipment, Khashab et al.,[13] reported the first human gastric peroral endoscopic myotomy and demonstrated the feasibility and efficacy of this approach. In a recent study [14], first European human endoscopic pyloromyotomy was performed in a female patient. At present, the therapeutic value of G-POEM has been attracting more and more attention, however, there is still no related report from China. In this operation, different from the previous reports, the submucosal tunnel was extended on the front gastric antral wall instead of the posterior wall. This approach has its own advantages: (1) this position may facilitate the extending of the tunnel. (2) It is safer to operate in front wall because there is no major internal organ in front of the stomach. Once a surgery was needed because of the complications such as hemorrhage and perforation, the front position could be more beneficial to operate. The patient has a vast improvement in gastro paretic symptoms noted at 3-month follow-up. This case further confirmed the reliability and availability of G-POEM. While the small number of cases certainly limits the widespread using. Operative methods, indications, and management of complications need more frequent use, increasing technical experience and the advantages of the front-wall tunnel need more data to confirm. Endoscopic pyloromyotomy has exciting potential to be at the forefront in the management of DGP.








































































































































