Gallbladder Hydrops
- 1. General Surgery, Hospital de especialidades Centro médico nacional La raza, México
- 2. General Surgery, Hospital General Regional, México
Citation
Vargas-Flores E, Beristain-Hernández JL, Velázquez-García JA, Ortega Román OA (2016) Gallbladder Hydrops. JSM Gen Surg Cases Images 1(1): 1002.
CLINICAL IMAGE
Elective cholecystectomy rarely presents with an acute biliary clinical entity, nevertheless it is a feasible surgical finding. Unaware diagnostic interpretation could lead to delayed treatment
A 16 years old teenager presents as an outpatient in a rural hospital complaining of chronic abdominal pain usually associated with cholecystokynectic meals. On physical exam, the patient does not reveal any signs of distress, abdominal focused examination shows mild pain exerted on deep right upper quadrant palpation without any obvious signs of peritoneal A 16 years old teenager presents as an outpatient in a rural hospital complaining of chronic abdominal pain usually associated with cholecystokynectic meals. On physical exam, the patient does not reveal any signs of distress, abdominal focused examination shows mild pain exerted on deep right upper quadrant palpation without any obvious signs of peritoneal availability on laparoscopic equipment) which occurred without any complication with surgical findings of gallbladder of 15x6 cm with distended and thin walls and mild inflammation. The patient underwent an uneventful recovery as it was discharged after 48 hours of in hospital surveillance.
Gallbladder hydrops is a rare clinical entity which appears to have a higher incidence among children. It is defined as an acute dilation of non-calculus origin, without inflammation but in some cases appears to be an obstruction of the cystic duct [1,3].Other pathologic entities should be discarded such as Kawasaki disease, mesenteric lymphadenitis, Leptospirosis, Mediterranean fever etc. All of which suggest it is a non-primary gallbladder pathology [1-4].

Figure 1 Gallbladder ultrasound showing an apparently normal gallbladder with a hyperechogenic image in the infundibulum.
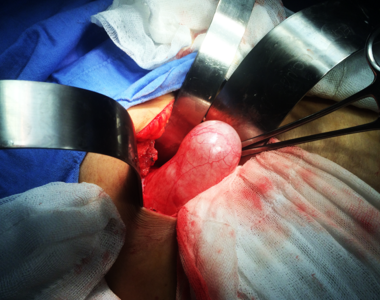
Figure 2 Exposure of gallbladder prior to dissection.
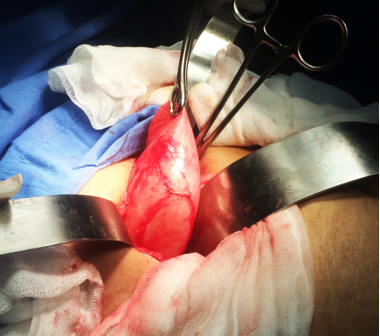
Figure 3 Traction of gallbladder after dissection of cystic artery and cystic duct.
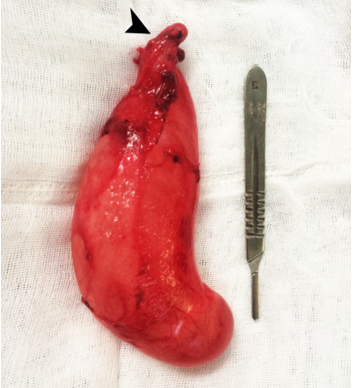
Figure 4 Extracted gallbladder. Black arrow shows obstruction of proximal cystic duct with a small stone.
Differential diagnosis should be made with acalculous cholecystitis, viral hepatitis, appendicitis and pancreatitis all of which should be always discarded [5]. Diagnosis is usually made during the operation with a distended gallbladder with signs of inflammatory involvement. Treatment is primary focused in conservative measures; nevertheless, cholecystectomy is also described. An uneventful recovery is usually present.








































































































































