Outcomes of Patients with Hyperkinetic Gallbladder: Does Surgery Relieve Symptoms
- 1. Department of Surgery and Department of Nuclear Medicine, St. John Hospital & Medical Center, USA
Abstract
Background: The purpose of this study was to investigate the outcomes of patients with hyperkinetic gallbladders; that is, ejection fractions (EF) greater than 80% on HIDA scan.
Methods: We reviewed the charts of all patients presenting to St. John Hospital & Medical Center with biliary pain who had a HIDA scan with EF >80% from January 1, 2000 to May 1, 2013. Patients agreeing to participate were asked questions from a standardized script over the telephone. Demographics, presenting symptoms, pain (on presentation and currently) and surgery date and satisfaction, if conducted, were recorded.
Results: 67 patients participated. Mean EF was 88.6 ± 5.0%. Fifty-eight (86.6%) patients did not have surgery. In these patients the initial pain score, (10 point scale), was 7.1 ± 1.9 vs. 4.1 ± 3.2, p<0.0005, at the time of the questionnaire. Nine (13.4%) patients had surgery, their initial pain score was 7.1 ± 1.8 vs. 2.0 ± 2.6, p=0.001 after surgery. Four (44.4%) of these patients had stones. We were unable to find a significant difference in the drop of pain score between those who had surgery and those who did not (p=0.067).
Discussion: Over time, some resolution of pain symptoms occurred in both groups (no surgery vs. surgery). The surgical group had a greater resolution of pain presented as a greater drop in pain score. The small number of patients who had surgery and the subjectivity of measuring pain scores limit our study. The presence of stones in the surgical group may also raise the possibility of under diagnosis of this problem.
Conclusion: Hyperkinetic gallbladders deserve further studies to understand its association with biliary pain and whether surgery should be offered to relieve this pain.
Citation
Afaneh A, Zhubi Y, Hagglund K, Kalabat J, Hawasli A (2016) Outcomes of Patients with Hyperkinetic Gallbladder: Does Surgery Relieve Symptoms? JSM Gen Surg Cases Images 1(4): 1016
INTRODUCTION
The nuclear HIDA scan with cholecystokinin (HIDA-CCK) has been a useful diagnostic tool in the work-up of patients with biliary pain/symptoms. In the absence of acute cholecystitis or symptomatic cholelithiasis, the ejection fraction (EF) can lend some information as to the etiology of the patient’s symptoms. After a HIDA scan for biliary pain, the ejection fraction is usually described as either normal (>35%) or indicative of biliary dyskinesia (<35%) [4]. A new term coined hyperkinetic or overactive gallbladder describes EF greater than 80% [2]. Biliary dyskinesia is typically treated successfully with laparoscopic cholecystectomy. There is little published information, however, on treating hyperkinetic or overactive gallbladder. Furthermore, there is little information in the literature as to the progression or outcomes of patients with biliary symptoms and hyperkinetic gallbladders. Some studies suggest that cholecystectomy may benefit patients with hyperkinetic gallbladders [2,3]. It is clear that the treatment of patients with hyperkinetic gallbladders is an area that requires further investigation. As more patients receive HIDA scans, the finding of Hyperkinetic gallbladder will become more prevalent and clinicians may find themselves encountering these patients. Our objective is to study the outcomes of these patients and to determine if surgery should be offered to provide relief.
RESEARCH QUESTION
Do patients with HIDA EF >80% benefit from laparoscopic cholecystectomy?
METHODS
We reviewed the charts of all patients presenting to St. John Hospital & Medical Center with biliary pain who received a HIDA scan from January 1, 2000 to May 1, 2013 with resulting EF >80% on HIDA. Medical records were accessed and an investigator attempted to reach the patients by telephone. Patients agreeing to participate and giving consent were asked questions from a standardized script over the telephone. Demographics, presenting symptoms, pain (on presentation and currently) and surgery date and satisfaction, if conducted, were recorded. See appendix 1 for a sample of the data reporting sheet. Medical record was accessed to record whether an ultrasound was previously done and if so, the presence or absence of stones was recorded. For patients who underwent surgery, if a pathology report was available, the results were noted as well.
RESULTS
The Nuclear Medicine Department found 286 patients who received HIDA scans with EF greater than 80% within our study period. The investigators then used electronic medical record to attempt to contact these patients. Many patients could not be contacted successfully while some refused participation in the survey. Sixty-seven patients participated in our study. Mean EF was 88.6 ± 5.0%. The mean age of the patients who participated in the study was 51 years old at the time of the survey. The age range was 22 to 83 years of age. 10/67 (15%) of the participants were male with 57/67 (85%) being female. Fifty eight (86.6%) patients did not have surgery. Pain symptoms on presentation were similar between both groups on a 10-pointe scale. The pain score was 7.1 ± 1.9 in the non-surgical group vs. 7.1 ± 1.8 in the 9 (13.4%) patients who had surgical removal of their gallbladder.
Documentation of ultrasound in the hospital records was found on 56/67 (83.6%) patients. The 11 (16.4%) patients whose ultrasound could not be found, all were in the non-surgical group. This leaves 47 patients in the non-surgical group with ultrasounds with only 3 (6.4%) found to have stones. None of these patients had surgery by the time of the survey. The remaining 44/47 of the patients, who did not have surgery and did not have stones on ultrasound, their initial mean pain score was 7.09 ± 1.9 on presentation. Four (44.4%) patients of the nine who had surgery had gallstones on ultrasound. The final pathology for these patients was “chronic cholecystitis”. For the five patients who had surgery and had no stones, their pathology included “no abnormality”, “chronic inflammation”, or “chronic cholecystitis”. One patient did not have a pathology report available as they had their surgery elsewhere (See (Table 1)).
|
Table 1: Operative group Results. |
|||||||
|
Patient |
EF |
Initial pain |
Present pain |
Resolution |
Satisfaction |
Stones |
Pathology |
|
1 |
86% |
7 |
3 |
Partial |
Satisfied |
Y |
Chronic cholecystitis |
|
2 |
91% |
4.5 |
0 |
Complete |
Very satisfied |
Y |
Acute on chronic inflammation |
|
3 |
93% |
8 |
0 |
Complete |
Very satisfied |
Y |
Chronic cholecystitis |
|
4 |
81% |
10 |
0 |
Complete |
Very satisfied |
Y |
Chronic cholecystitis |
|
5 |
80% |
8 |
8 |
None |
Dissatisfied |
N |
N/A |
|
6 |
90% |
5 |
0 |
Complete |
Very satisfied |
N |
Chronic inflammation |
|
7 |
86% |
5 |
2 |
Partial |
Satisfied |
N |
Chronic cholecystitis |
|
8 |
83% |
8 |
2 |
Partial |
Very satisfied |
N |
Chronic cholecystitis |
|
9 |
85% |
8 |
3 |
Partial |
Very satisfied |
N |
No abnormality |
Over time, resolution of pain occurred in both groups. At the time of the survey, the surgical group had less pain as evidenced by the further decrease in their pain score in comparison to the non-surgical group : 2.0 ± 2.6 vs. 4.1 ± 3.2 (p =0.067) . It was interesting to find that 24 patients (41.4%) in the non-surgical group had either complete resolution of pain (14 patients) or significant resolution (10 patients) (See (Figure 1)).
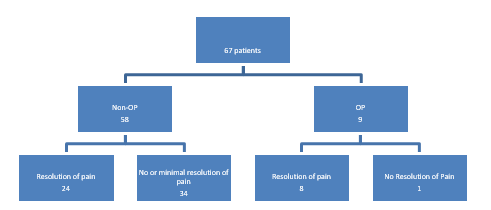
Figure 1 Results.
Significant resolution of pain was defined as a drop in pain score by more than 50% of the original score. This was contrasted in the surgical group where all but one patient had resolution of pain
DISCUSSION
The goal of our study was to look at the outcome of patients with hyperkinetic gallbladders. These patients have not been studied well because traditionally an ejection fraction greater than 35% was deemed normal. Our study aimed to investigate these patients and see what the progression of their symptoms was. Our results demonstrate that although there is a drop in pain score in both groups, the surgical group demonstrated a larger drop in pain score. However, the difference in the drop of pain score between the two groups was not significant (p=0.067).
Our study is limited by the small number of patients with hyperkinetic gallbladders who underwent surgery. Only nine of the 67 patients had surgery. Four of these 9 patients had stones on ultrasound and one can argue that this may bias our results. Only 5 patients who had hyperkinetic gallbladders and no stones underwent surgery. In four of these five patients the pain symptom was significantly resolved. The small number of patients who underwent surgery again limits our results. This low number of patients undergoing surgery is not surprising because patients with high ejection fractions were not traditionally offered any kind of intervention and surgery is not viewed as a standard of care. Clinicians are probably more likely to offer surgery to patients with stones whether or not their ejection fraction is high. For the patients who do not have stones and have hyperkinetic gallbladder, the options have been traditionally limited and centered on symptomatic relief of pain by medical management.
Many of the patients interviewed did not have surgery and continued to have symptoms. It would be interesting to see how many of these patients would consider surgery as an option to alleviate their symptoms. One may argue, however, that in 41.4% of patients who did not have surgery, they experienced either complete or significant resolution of their pain over time. This means that a significant number of patients may not need surgery to relieve their symptoms. The significant number of patients in the non-surgical group with resolution of pain points to the possibility that this condition may be transient or self-limiting.
A large randomized prospectively controlled study is needed in which symptomatic patients with no stones and hyperkinetic gallbladders are offered surgery to possibly relieve their symptoms.
CONCLUSIONS
Resolution of pain symptoms in patients with hyperkinetic gallbladder occurred in both groups (no surgery vs. surgery). The surgical group had a greater resolution of symptoms and drop in pain score, although this difference was not significant (p=0.67). The small number of patients who had surgery, as well as, the subjectivity of measuring pain score limits our study. A large prospective study is needed in which patients with hyperkinetic gallbladders and no stones are offered laparoscopic cholecystectomy to help alleviate their symptoms.








































































































































