Presacral Cystadenocarcinoma after Persistent Perineal Sinus
- 1. Department of Surgery, Hospital Universitario Marqués de Valdecilla, Spain
- 2. Department of Surgery, Hospital Universitario Marqués de Valdecilla, Spain
Abstract
Presacral Tumours are a rare entity. Diagnosis is difficult and surgical treatment is often a real challenge. Occasionally, because of nonspecific clinical appearance and the difficulty of a biopsy, it’s impossible to make an accurante diagnosis before treatment.
Keywords
• Retrorectal tumour
• Rectal cancer
• Presacral tumour
Citation
Poch LC, Gomez- Ruiz M, Fernandez CC, Mayorga M (2016) Presacral Cystadenocarcinoma after Persistent Perineal Sinus. JSM Gen Surg Cases Images 1(1): 1004.
INTRODUCTION
Aim
Present a clinical case of cistoadenocarcinoma developed after abdominopertoneal resection (APR) for a low rectal tumor.
CASE PRESENTATION
Methods
A 73- year-old man presented to our Colorectal Office, with a persistent perineal sinus. He had previously undergone an abdominoperineal resection (APR) in 2010. He provided reports from another hospital, where we could clarify that the pathological study of the specimen of 2010 was benign. He suffered with persistent discharge and pelvic pain, progressing over the last years. CT-Scan and pelvic MRI were performed as well as a Fine needle aspiration biopsy (FNAB)
Results
The radiology study showed a collection above the surgical wound and PET scan showed a normal distribution of the radioactive tracer. FNAB indicated absence of malignant cells a posterior Kraske approach was indicated with resection of the coccyx. A big cystic pelvis mass (Figure 2)

Figure 2 Cyst with rough walls, mucinous aspect, and solid areas.
was found, affixed to rear face of the bladder and prostate, entering the vas deferens. An en bloc resection and a simultaneous staged pedicle V-Y was madewith an uneventful postoperative course. Pathology results came with Cystadenocarcinoma, free margin. Adjuvant therapy based on chemo-radiation was recommended as decided in the multidisciplinary committee.

Figure 1 In the surgical site there is a lobed abscess of 10, 5 x 7 x 7 cm.
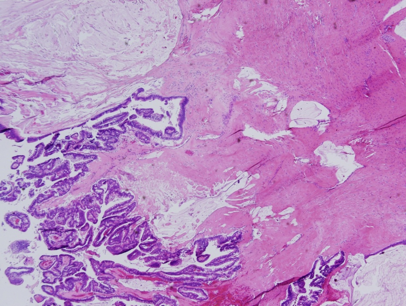
Figure 3 Histology shows a thin capsule, cystic structures lined with columnar glandular epithelium.
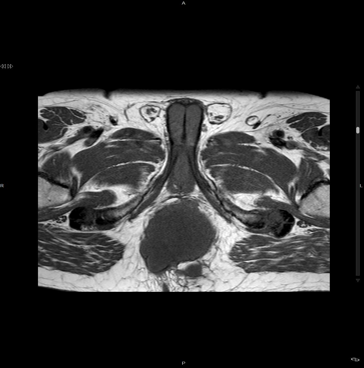
Figure 4 Magnetic resonance imaging (MRI) of the pelvis.

Figure 5 Magnetic resonance imaging (MRI) of the pelvis. T1W1.
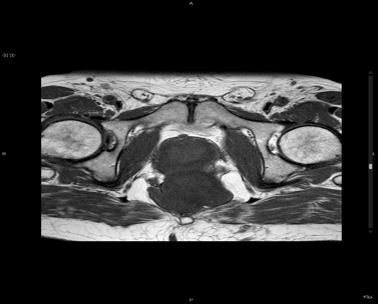
Figure 6 cyst with rough walls, mucinous aspect and solid areas.
DISCUSSION
Retro rectal tumours are un common, the clinical presentation is heterogeneous, ranging from chronic non-specific abdominal pain, constipation, bowel obstruction, to suppuration. The definitive treatment is surgical, because of the risk of misdiagnosis or malignant degeneration.








































































































































