Valuable Experience of a Missed Spontaneous Duodenal Fistula Resulting in Complete Duodenal Occlusion in Severe Acute Pancreatitis.
- 1. Department of Hepatobiliary Surgery, Zhongshan Hospital of Xiamen University, China
- 2. Department of Hepatobiliary Surgery, Zhongshan Hospital of Xiamen University, China
Abstract
Severe acute pancreatitis (SAP) is a devastating disease that is characterized with high mortality due to the development of Local or systemic complications, such as infected pancreatic and extra-pancreatic necrosis (IPN), multisystem organ failure. Gastrointestinal fistula (GIF) is a well-recognized complication secondary to SAP and has been attracting much attention. But complete duodenal occlusion (CDO) is an extremely rare complication secondary to GIF in patients with SAP. In this paper we describe a case of missed spontaneous duodenal fistula resulting in CDO in patients with SAP
Keywords
• Severe acute pancreatitis
• Gastrointestinal fistula
• Duodenal fistula
• Complete duodenal occlusion
Citation
Hua Z, Su Y, Huang X, Pro ZY, Pro XW, et al. (2017) Valuable Experience of a Missed Spontaneous Duodenal Fistula Resulting in Complete Duodenal Occlusion in Severe Acute Pancreatitis. JSM Gen Surg Cases Images 2(1): 1020.
INTRODUCTION
Severe acute pancreatitis (SAP) is a devastating disease that affects thousands of patients annually and leads to substantial mortality. It has a complicated clinical course with higher risks for prolonged hospitalization and healthcare costs. The high mortality ranges up to 20% make SAP among the most lethal of all gastrointestinal (GI) diseases [1,2]. Gastrointestinal fistula (GIF) is one of the well-recognized complications in SAP. It may result from direct erosion from digestive enzymes released by the inflamed pancreas on adjacent GI tract, or it can occur as a consequence of the intestinal necrosis due to vascular thrombosis in an area of inflammation and infection. Additionally, GIF may also be complicated with surgical intervention [3]. Depending on the sites of fistula, GIF may involve the stomach, duodenum, jejunum, ileum, and colon, either in combination or separately. It has been reported that most upper-gut fistulas could usually close spontaneously with time if infected source could be well controlled and colonic fistulas may require active intervention [4,5]. It is undeniable that GIF may cause serious clinical consequences, such as hemorrhage and exacerbation of infections, which can lead to a fatal outcome [6]. GIF involvement is difficult to diagnose clinically and radiologically due to potential symptoms caused by ischemic and/or reactive peritonitis that are usually overlaid by the symptoms of SAP. Obtaining a computed tomography (CT) scan is the first step in diagnosing a GIF. Indeed, the presence of air densities in the necrotic cavity is an important diagnostic feature on the CT scan. Other diagnostic modalities used for GIF are often based on fistulography, digestive endoscopy, or operative findings [7]
CASE REPORT
A 51-year-old male was referred to our hospital with a complaint of colicky pain, localized in the periumbilical area with radiation to the back, accompanied with nausea and vomiting after imbibing a large amount of alcohol the evening prior to admission. He was admitted with SAP to the intensive care unit after contrast-enhanced computed tomography (CECT) demonstrated the presence of pancreatic necrosis that occupied the whole pancreatic parenchyma and was accompanied by peripancreatic fluid collection (Figure 1a).
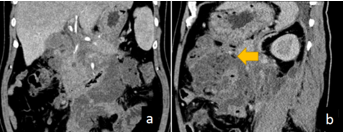
Figure 1 CECT scan of the abdomen showing acute infected necrotizing pancreatitis: a massive area of necrosis in the peripancreas and bilateral retroperitoneal peripancreatic necrosis containing an air bubble (yellow arrow) can be seen; this raised the suspicion of infected pancreatic necrosis and/or fistula formation.
The patient subsequently developed systemic inflammatory response syndrome requiring intubation, and acute renal injury requiring hemodialysis. A follow-up CECT after 2 weeks revealed aggravation of the peripancreatic necrosis with air densities (Figure 1b). The patient had also complained of recurrent episodes of melena with severe anemia. After blood transfusion many times, his situation improved. Percutaneous catheter drainage tubes were placed in the cavity of the peripancreatic necrosis, and retroperitoneal laparoscopic debridement drainage was performed twice, while in addition laparoscopic trans-retroperitoneal debridement and necrosectomies together with jejunostomy were performed successively combined with postoperative persistent washing and drainage. The patient’s condition improved markedly but he was not able to eat a normal diet due to distension, and he was provided with enteral nutrition mainly via tube by jejunum feeding. Gastroduodenoscopy (Figure 2)
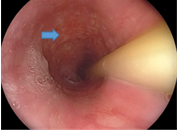
Figure 2 Gastroduodenoscopy images revealing the edematous wall on the pancreatic side of the lower descending duodenum (blue arrow).
and upper gastrointestinal radiography (Figure 3)
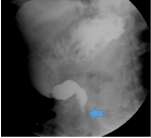
Figure 3 Gastroduodenography imaging with Diatrizoate demonstrating marked stenosis, almost resulting in atresia of the distal descending duodenum (blue arrow).
confirmed the presence of a completely impassable duodenal stricture. Six months later, refractory duodenal obstruction persisted and resulted in luminal stenosis, revealed by duodenoscopy (Figure 4).
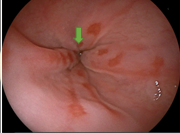
Figure 4 Gastroduodenoscopy images showing changes resulting from a series of processes such as corrosion, thrombosis, ischemia, necrosis, perforation, fistula, and ultimately, formation of adhesive atresia (green arrow).
Gastro-jejuno anastomosis was then performed, and during the operation, an inflammatory mass surrounding and adhering to the horizontal part of the duodenum was observed. Two weeks later a gastrointestinal anastomotic fistula was found; fortunately, leak closure was achieved after another 2 weeks following the removal of fistula drainage. Finally, the patient was discharged on a normal diet on the 243rd hospital day.
DISCUSSION
Though significant progress has been made over the past 20 years in the management of circulatory dysfunction and multiple organ dysfunctions in SAP. [8,9] However, treatments of GIF usually are managed conservatively and the role of intervening procedures is controversial[10]. Complete duodenal occlusion (CDO) secondary to SAP with GIF are reported rarely in the literature yet are followed with severe sequelae and catastrophic mortality. In this paper we provided valuable experience of the treatment of a missed duodenal fistula subsequent to persistent duodenal occlusion in a case of SAP.
GIF is suspected if there are air pockets visible within the necrotic area on CECT, but these are easily confused with air bubbles caused by the infection of peripancreatic necrosis [11]. In this case, acute necrotizing pancreatitis associated with occult duodenal fistula was hard to find, and the missed diagnosis meant that the fistula had failed to be treated in a timely and effective manner. Only when the patient’s inability to eat and anorexia necessitated further examination did gastroscopy confirm completely impassable duodenal stenosis/CDO. During later surgery, an inflammatory process with a mass was discovered, which encompassed and depressed the distal portion of the descending duodenum posterior to the head of the pancreas. The granulated mucosa of the duodenal wall embedded in the mass was presumed to be the sequela of a localized duodenal fistula, which was confirmed by the recurrent episodes of melena and bile in the drainage fluid. Biopsy confirmed the absence of malignancy. Gastro-jejuno anastomosis was performed necessarily and followed by the principles of damage-control surgery in this frail and critical patient who would not tolerate more aggressive surgery.
The main point of treatment of duodenal fistula is to overcome sepsis by evacuation of pus, involve endoscopic or percutaneous external drainage of intra or extra-luminal collections, decompression of the duodenum, and provision of enteral nutritional support (feeding jejunostomy) is very important. Surgical choice and modalities depends on the availability of expertise and the severity of comorbid medical illness. Minimally invasive strategies are being more recommended by gastrointestinal surgeons, radiologists, and gastroenterologists, as well as the rationales of interventional management of infected necrotizing pancreatitis in SAP [10,12,13].
It seems likely in this case that the complication of CDO and the almost 8-month hospital stay could have been avoided with earlier gastroduodenoscopy and interventions with drainage of the fistula. Evidences of repeated episodes of melena with severe anemia and bile in the drainage fluid, which were considered to be complications of bile leakage in IPN and haemorrhage result from stress ulcers, and did not cause enough attention. And the critical situation of the patient prevented to administrate earlier endoscopy examination for an early diagnosis and treatment of the fistula. All of which led to the deterioration of the condition and the regrettable outcome finally.
It is inevitable to occur defects in the diagnosis and treatment of GIF because of which involved with complex and recondite processes. Nevertheless, optimal prospective validation and utility studies are urgently required to provide confidence in the diagnosis and treatment of lethal complications of SAP and thus to improve decision making








































































































































