Effect of Self-Esteem Components and Parental Monitoring on Cannabis use Among American Indian Adolescents
- 1. Department of Psychology, Colorado State University, USA
Abstract
This study examined mediating effects of internal and external self-esteem on the relationship between components of parental monitoring and cannabis use among American Indian (AI) adolescents. A total of 4056 American Indian 7-12th grade students attending 42 schools on or near reservations completed the Our Youth, Our Future survey. The data were collected in 2018-2019 as part of an ongoing epidemiological, population-based study of AI youth. Exploratory and confirmatory factor analyses (EFA, CFA) of self-esteem were conducted, followed with mediation model testing. Four measures of parental monitoring were taken from the Parental Monitoring Short Scale (PMSS; total scale, parental knowledge, parental control, child disclosure/parental solicitation). The EFA and CFA results supported two factors of self-esteem: internal and external. All parental monitoring components related negatively to cannabis use. Additionally, all parental monitoring components were indirectly related to cannabis use through internal, but not external self-esteem. The results indicate that external self-esteem may not impact effects of parental monitoring on substance use among AI adolescents while internal self-esteem does. Further study of self-esteem interventions is indicated as potentially enhancing influences of parental monitoring on adolescent cannabis use along with other majority and ethnic minority adolescents to determine if these results extend beyond AI youth.
Keywords
• Cannabis
• American Indian
• Adolescents
• Self-esteem
• Parental monitoring
• Mediation
Citation
Swaim RC, Haruyama D, Prince MA, Chavez EL (2025) Effect of Self-Esteem Components and Parental Monitoring on Cannabis use Among American Indian Adolescents. J Addict Med Ther 12(1): 1049.
INTRODUCTION
Cannabis is the second most commonly used substance among U.S. adolescents [1]. Early initiation of cannabis increases risk for development of a cannabis use disorder [2], and adolescent cannabis use increases the likelihood of risk for abuse and dependence of other illicit drugs [3]. Among those who begin cannabis use in adolescence versus adulthood, risk is two to four times more likely for development of cannabis dependence symptoms within 24 months after first use [4]. Reservation-dwelling American Indian (AI) adolescents are at highest risk for cannabis use, reporting 4.2, 2.5, and 1.7 times more use in the last 30 days than U.S. youth across 8th, 10th, and 12th grades respectively [5].
Furthermore, they initiate use much earlier than their White counterparts attending the same schools [6]. These findings emphasize the importance of identifying, more clearly, those factors that relate to cannabis use among AI youth. In this study we focus on two factors examined extensively in the literature in relation to adolescent substance use: self-esteem and parental monitoring. Specifically, we examine the potential mediating effects of self-esteem on the relationship between parental monitoring and cannabis use among this group of at-risk adolescents. While limited in number, results from past research investigating self-esteem in relation to AI substance use are mixed.
In a longitudinal six-wave study of AI high school students from four culturally distinct reservations, Whitesell, Mitchell, Spicer, and The Voices of Indian Teens Project Team [7], found that growth in self-esteem from Waves 2-4 was associated with less substance use and less antisocial behaviors at Wave 5. In contrast, among 5th through 8th grade AI youth, self-esteem failed to relate to a measure of resilience that included lower substance use [8]. Swaim and Stanley [9], examined whether self-esteem might moderate the effects of cultural identification on alcohol and marijuana use among AI youth from 46 schools on or near reservations. But no moderating relationship was found.
Two measurement factors may help explain these conflicting results. First, Swann, Chang-Schneider, and McClarty [10], argue that self-esteem, as a global predictor, may not be associated with specific outcomes such as substance use. Second, in each of the studies cited, a global measure of self-esteem was used. Swaim and Wayman [11], examined the factor structure of a nine-item measure of self-esteem and identified three factors: self-confidence, competence, and social acceptance. When examined in relation to alcohol use among Mexican American and White non-Latino ninth- and tenth-grade adolescents, competence and self-confidence were each negatively related to alcohol use, except among Mexican American females. However, when followed up two years later, only one prospective relationship was found, with lower selfconfidence at Time 1 associated with higher alcohol use at Time 2.
These results suggest that differing components of self-esteem may relate differentially to adolescent substance use. This was confirmed in a study by Schick, Nalven, and Spillane [12], among AI adolescents. With an extended 11-item self-esteem scale, they identified two factors: internal (IN) and external (EX) self-esteem. IN (a composite of Swaim & Wayman’s self-confidence and competence) related negatively to alcohol and alcoholrelated problems, while EX (Swaim & Wayman’s social acceptance) related positively to these variables. Thus, it may be important to consider each of these components of self-esteem individually. While the relationship between self-esteem and substance use is likely complex, it may be altered by parental monitoring. A higher level of parental monitoring is associated with lower levels of substance use [13- 15]. In a study of reservation AI youth, higher levels of parental monitoring were associated with less likelihood of lifetime cigarette smoking and cannabis use. However, these results were found only among female youth [16]. Additionally, higher levels of parental monitoring are associated with higher levels of self-esteem in adolescents [17-19].
However, some studies failed to find a positive relationship between parental monitoring and self-esteem [20-22]. To date, the relationship between parental monitoring and self-esteem has not been identified in AI adolescents. Other studies found that self-esteem serves a mediating role between parenting behaviors and adolescent outcomes. For example, Wouters, Colpin, Luyckx, and Verschueren [23], found in a sample of Dutch adolescents that self-esteem mediated the effects of perceived parental control on internalizing symptoms, including depression and anxiety. Similar findings were reported for Turkish adolescents for whom self-esteem mediated the effects of parental monitoring (knowledge) on antisocial behavior [24]. Among 5th and 8th-grade students, Hunter, Barber, and Stolz [25], found that positive self-esteem mediated the effects of psychological control (manipulative, guiltinducing) on depression and antisocial behavior (not including substance use). But self-esteem did not provide mediating effects between behavioral control (parental knowledge of child behaviors) and these outcomes. However, positive self-esteem in this study was measured as a global construct. Based on these previous findings, this study evaluates the potentially complex mediating effects of two subcomponents of self-esteem (IN and EX) on the relationship between various components of parental monitoring (knowledge, parental control, child disclosure/ parental solicitation) on cannabis use among a populationbased sample of AI adolescents attending schools on or near reservations.
The results by Schick et al. [12], suggest that IN self-esteem may serve a mediating role, while EX self-esteem may not. Findings from Wouters et al. [23], Hunter et al. [25], and Özdemir et al. [24], support the mediating role of self-esteem on different components of parental monitoring (control and knowledge), but their studies were limited by use of a global measure of selfesteem. This study contributes to the adolescent substance use literature by investigating more fully the complex relationships between different components of self-esteem and parental monitoring factors in relation to cannabis use among reservation-dwelling AI youth.
MATERIALS AND METHODS
Participants
Data are from cross-sectional surveys collected during 2018-2019, part of an ongoing epidemiologic study of AI youth living on or near reservations. Schools were randomly drawn from a sampling frame of 382 schools that contained a grade 7. These schools were stratified into seven geographic cultural regions unique to AIs in the continental U.S. (Northeast, Northwest, Southwest, Northern Plains, Southern Plains, and Upper Great Lakes). When a school containing a grade 7 agreed to participate, the high school that received students from this school was recruited for participation. The final sample consisted of 7-12th grade students self-identifying as AI from 42 schools (n=4056; 48.7% female; 50.6% male; 0.3% did not answer). Mean age was 14.5 (SD = 1.79). The mean percentage of students eligible for free or reduced lunch was 74.5% with 14 schools having 100% of students eligible.
Procedure
The study was approved by the University IRB. For each participating school, the appropriate tribal and school board approvals were also obtained. Upon school agreement to participate, parents were sent a notification about the study with instructions on how to opt their child out. Less than one percent chose this option. The surveys were completed online during a class period using the Qualtrics platform. All surveys were completed anonymously. At the beginning of the survey, students were asked to assent to taking the survey while being instructed that they could decide not to take the survey or could not answer questions with which they were not comfortable responding. Each participating school received a comprehensive report of their survey findings and compensation for resources used to complete the survey process depending on size of school (median payment, $1500).
Measures
Parental Monitoring. Parental Monitoring was measured with the Parental Monitoring Short Scale as shown in Table 1 [26]. This scale is a revised and shortened version of the measure developed by Stattin and Kerr [27], along with items measuring parental knowledge. These items were factor analyzed with an AI and White sample and yielded three factors, with three items each: parental knowledge (PK, alpha=.91; parental control (PC, alpha=.86; child disclosure/parental solicitation (CD/PS, alpha=.89). It should be noted that the factor analysis resulted in the combined factor, CDPS, while these were two separate factors according to Stattin and Kerr. Response categories for the PMSS items were 1=Never, 2=Rarely, 3=Sometimes, 4=Most of the time, and 5=Always.
Table 1: Parental Monitoring Short Scale.
|
|
Parental Knowledge |
|
1 |
My parents know where I am after school. |
|
2 |
When I go out at night, my parents know who I am with. |
|
3 |
When I go out at night, my parents know where I am. |
|
|
Parental Control |
|
4 |
I need permission to be out late on weeknights. |
|
5 |
I have to tell my parents who I’m with and what I’m doing at night with friends. |
|
6 |
I have to tell my parents my plans for weekend nights. |
|
|
Child Disclosure/Parental Solicitation |
|
7 |
My parents talk to my friends. |
|
8 |
My parents ask me what I do in my free time. |
|
9 |
My parents ask about things that happen at school. |
|
10 |
I tell my parents about my activities with friends. |
|
11 |
I tell my parents how I’m doing in school |
|
12 |
I keep secrets from my parents about what I do in my free time. |
|
Note: Item 12 was removed from the CD/PS scale due to poor psychometrics. |
|
Self-esteem (SE). The self-esteem measure was originally developed by Swaim, Oetting, Edwards, and Beauvais, [28], and was validated with AI youth [9]. It consists of 11 items designed to measure three components of self-esteem: self-confidence, competence, and social acceptance (alpha=.80; in Table 1). Response categories for this measure were 1=Not at all, 2=Not much, 3=Some, and 4=A lot. As noted earlier, two factors were identified in a sample of AI youth: intrapersonal (e.g., “I like myself,” alpha=.83), and interpersonal (e.g., “Other people like me,” alpha=.84). Current cannabis use. The criterion variable for the study was current cannabis use, assessed with the question, “How many times (if any) have you used cannabis (weed, pot) or hashish (hash, hash oil) during the last 30 days?” Participants chose among seven possible responses: 0=0 times, 1=1-2 times, 2=3-5 times, 3=6-9 times,4=10-19 times, 5=20-39 times, and 6=40 or more times.
Statistical Analysis
Factor analysis of SE. As Swaim and Wayman [11], originally identified three factors for SE, in contrast to the two factors identified by Schick et al. [12], an EFA was conducted to confirm the factor structure with the current sample. Comparisons were made across one, two, and three factor models, followed by a CFA for the best fitting model. Mediation Analysis. Separate tests of mediation were conducted across sub-factors of parental monitoring (parental knowledge, parental control, child-disclosure/ parental solicitation). Multiple mediation tests were examined with both IN and EX self-esteem serving as potential mediators of the relationship between components of parental monitoring and current cannabis use.
Figure 1 presents an example of a mediational model for parental knowledge. Because the data were crosssectional, we used atemporal mediation analysis [29]. Mediation was tested using path analysis with Mplus 8.1 [30]. Because current cannabis use was highly positively skewed with a floor effect (i.e., with most participants selecting the lowest value of “0 times” in the last month), we used negative binomial regression with Bayesian Credibility Intervals (BCI) to determine statistical significance. BCI uses a posteriori probability approach whereby the data already obtained is used to calculate the distribution of the probability of different values [31]. If at 95% these credibility intervals do not contain zero, they are considered statistically significant. Unstandardized paths leading to cannabis use were exponentiated to calculate rate ratios (RR).
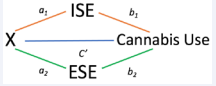
Figure 1 Figure presents an example of a mediational model for parental knowledge Note: X represents the independent variables of PM, PK, PC and CD ISE refers to self-esteem from beliefs about internal qualities (i.e., intrapersonal SE) ESE refers to self-esteem from beliefs about external perspectives on self (i.e., interpersonal SE)
FINDINGS
Descriptive Statistics
Descriptive statistics are presented in Table 2 for demographic variables, cannabis use, IN and EX selfesteem, and sub-components of parental monitoring.
Table 2: Descriptive Statistics of Key Variables.
|
|
Mean |
SD |
Min |
Max |
|
Grade |
9.03 |
1.67 |
7 |
12 |
|
Age |
14.61 |
1.75 |
11 |
21 |
|
Sex |
1.49 |
0.16 |
1 |
2 |
|
Cannabis Use |
0.83 |
1.75 |
0 |
6 |
|
Internal Self-Esteem |
3.13 |
0.87 |
1 |
4 |
|
External Self-Esteem |
2.84 |
0.84 |
1 |
4 |
|
Parental Monitoring |
3.50 |
0.95 |
1 |
5 |
|
Parental Knowledge |
4.22 |
1.10 |
1 |
5 |
|
Parental Control |
3.63 |
1.22 |
1 |
5 |
|
Child Disclosure/ Parental Solicitation |
3.05 |
0.98 |
1 |
5 |
|
Note: Cannabis use (last 30 days); Parental Monitoring (full scale). |
||||
Factor Analysis for Self-Esteem
The initial EFA included all eleven SE items and compared model fit and factor loadings of one, two, and three factor structures (Table 3). Each inclusion of an additional factor improved fit suggesting that the threefactor model was the preferred solution. However, when examining the oblique GEOMIN rotation, recommended when items have substantial loadings on more than one factor [32], one item (“I am good looking”) loaded on two factors with a higher loading on Factor 2. This left only two items with loadings greater than .4 for Factor 3. Therefore, the two-factor solution was selected as the best fitting model. Examination of the items for these two factors suggested that they reflected internal self-esteem (IN) and external self-esteem (EX).
Table 3: EFA Comparing 1, 2, and 3 Factors for Self-Esteem.
|
Model |
Parameters |
Chi-square |
df |
p-value |
RMSEA |
CFI |
SRMR |
|
1 Factor |
33 |
5069.27 |
44 |
<.001 |
0.175 |
0.789 |
0.071 |
|
2 Factor |
43 |
926/07 |
34 |
<.001 |
0.084 |
0.962 |
|
|
3 Factor |
42 |
343.51 |
25 |
<.001 |
0.058 |
0.987 |
0.017 |
|
Models Compared |
|||||||
|
|
|
Chi-square Δ |
df |
p-value |
|
|
|
|
1 vs. 2 Factor |
4143.19 |
10 |
<.001 |
|
|
|
|
|
2 vs. 3 Factor |
582.56 |
9 |
<.001 |
|
|
|
|
model. Examination of the items for these two factors suggested that they reflected internal self-esteem (IN) and external self-esteem (EX). Next, the two-factor structure items were removed one at a time for items that did not load strongly onto either factor. Items were removed in the following order: “I am good at games,” “I am good looking,” “I am lucky,” “I am smart,” and “Other people my age ask me to do things with them.” This resulted in a final scale with three items each on IN and EX. The final factor loadings for IN ranged from .77 to .97 and the final factor loadings for EX ranged from .84 to .87. A CFA was conducted on the six-item scale and model fit indices indicated a good fit (RMSEA=.047; CFI=.99; SRMR=.016).
Mediation Model Testing
Parental Monitoring (PM). PM was directly and positively related to both IN (b=0.33, SE= 0.01, p<.01) and EX (b= 0.28, SE= 0.01, p<.01). PM was also directly and negatively related to CU (RR = .66, b= -0.42, SE= 0.05, p<.01). Additionally, PM was indirectly related to CU through the IN pathway (ind = -0.06, BCI = -.10, -.27), but not through the EX pathway (ind = 0.02, BCI = -.01, .04). In this and all subsequent models, male students reported higher levels of IN and EX and older students reported higher levels of CU. Parental Knowledge (PK). PK was directly and negatively related to CU (RR = .70, b = -0.36, SD= 0.05, p<.01). PK was also positively related to IN (b = 0.25, SE= 0.01, p<.01) and EX (b = 0.20, SE= 0.01, p<.01). PK was indirectly related to CU through the IN pathway (ind = -.05, BCI = -.08, -.02), but not through the EX pathway (ind = .01, BCI = -.01, .03).
Parental Control (PC). PC was directly and negatively related to CU (RR = .72, b = -0.33, SD= 0.04, p<.01). PC was also directly and positively related to both IN (b= 0.20, SE=0.06, p<.01) and EX (b = 0.17, SE= .01, p<.01). PC was indirectly related to CU through the IN pathway (ind = -0.04, BCI = -.07, -.02), but not the EX pathway (ind = .01, BCI = -.01, .03). Child Disclosure/Parental Solicitation (CDPS). CDPD was directly and negatively related to CU (RR = .73, b= -0.31, SD= 0.05, p<.01). CDPS was also directly and positively related to both IN (b = 0.31, SE= 0.01, p<.01) and EX (b = 0.27, SE= 0.01, p<.01) CDPS was indirectly related to CU through the IN pathway (ind = -0.06, BCI = -.09, -.02) but not the EX pathway (ind = .01, BCI = -.01, .05).
DISCUSSION
Reservation-area AI students are at high risk for cannabis use compared to national youth [5]. Past research indicates that parental monitoring is protective against AI substance use [33-34], with results for protective effects for global self-esteem being mixed [7,8]. However, previous studies of both parental monitoring and selfesteem used measures that overlooked nuances in the relationship between subdomains of these factors. We examined relationships that included parental knowledge, parental control, and child-disclosure/parental solicitation for parental monitoring, and internal and external selfesteem. Specifically, we tested whether the effects of various components of parental monitoring on cannabis use would be mediated through internal and external selfesteem. First, and consistent with past research [17,19], we found that among AI reservation-area adolescents, parental monitoring was positively associated with both internal and external self-esteem. This relationship held for the overall measure of parental monitoring and each of its subdomains. This relationship was slightly stronger between the measures of self-esteem and child-disclosure/ parental solicitation.
Student willingness to share personal information with parents may be more likely among higher self-esteem youth due to higher personal resources for vulnerability and transparency [35]. We also found that all measures of parental monitoring were significantly related negatively to recent use of cannabis. This too is consistent with past findings of the protective effects of parental supervision and control against substance use among youth in general [13,15], and among AI youth [16]. This is also supported is a previous study by Eitle et al. [36], which social resources in the form of parental control buffered the effects of negative life events on substance use among AI adolescents. Also of interest in this study was the comparison between AI and non-Hispanic White students on perceived parental control. Given American Indian families’ value for providing their children with independence and autonomy in decisionmaking [37,38], we considered that parental control might not be substantially related to substance use among our sample of Indigenous youth. However, Eitle et al. [36], found no difference in perceived autonomy between their samples of AI and non-Hispanic White youth.
This suggests that when it comes to child misbehavior, there may not be substantial differences between AI and non-AI parenting regarding child autonomy. The direct relationships we observed set the stage for our primary question, whether components of selfesteem would mediate the negative relationship between monitoring and current cannabis use. Findings were consistent across all measures of parental monitoring. In each case, the monitoring measure was indirectly related to cannabis use through IN self-esteem, but not through EX self-esteem. As noted previously, prior research has not made a distinction in these two subdomains of selfesteem, but instead used a global measure. This is the first study to identify a unique aspect of self-esteem that serves the mediating function between monitoring and substance use.
The finding for internal self-esteem, however, is not surprising. Most measures of global self-esteem largely measure internal self-esteem. For example, the Rosenberg Self Esteem Scale [39], primarily measures one’s internal appraisal of self. Representative items include, “On the whole I am satisfied with myself,” and “I take a positive attitude toward myself.” Thus, one important finding of our results is that external self-esteem does not substantially impact the effect of parental monitoring on substance use. It is important to note that our measure of external selfesteem does not tap positive parental attitudes toward their children. We suspect that the source of external selfesteem for these AI youth is likely to come from appraisal of their peers with items such as, “People like me,” and “Other people ask me to do things with them.” Further work should explore the extent to which self-esteem promoted through parent-child interaction may compare for its protective effects as compared to other social sources of self-esteem that are internally based.
CONCLUSIONS, LIMITATIONS & RECOMMENDATIONS
These findings broaden the scope of this literature for which results regarding various components of parental monitoring and mediation through aspects of self-esteem are scarce. Interventions that target improvement of youth self-esteem are effective and can also impact reductions in externalizing behaviors such as substance use [40]. Our results point to the need for further study of self-esteem interventions as means to enhance the positive influence of parental monitoring on adolescent cannabis use and other forms of substance use. The findings presented should be considered in light of the limitations of the study design and sample.
While this study includes a large sample of reservation-dwelling youth, it does not include other Indigenous people including urban Natives or Indigenous people who do not live on or near reservations. Further, as the data are cross-sectional, we were limited to examining atemporal mediation methods, which provide critical information about the relation between the predictor and outcome variables when accounting for the shared relation among all variables in the model but precludes evidence for a causal chain. Taken together, the present study adds to the existing literature on parental monitoring, self-esteem, and cannabis use among AI youth. Further study should evaluate whether these findings can be replicated in other populations and extended with longitudinal research.
REFERENCES
- Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the Future national survey results on drug use, 1975–2021: Secondary school students. Ann Arbor: Institute for Social Research, The University of Michigan. 2022; 1.
- Volkow ND, Baler RD, Compton WM, Weiss SRB. Adverse health effects of marijuana use. NEJM. 2014; 370: 2219-2227.
- Fergusson DM, Boden JM, Horwood LJ. The developmental antecedents of illicit drug use: Evidence from a 25-year longitudinal study. Drug Alcohol Depend. 2008; 96: 165-177.
- Chen CY, Storr CL, Anthony JC. Early-onset drug use and risk for drug dependence problems. Addict Behav. 2009; 34: 319-322.
- Swaim RC Stanley LR. Substance use among American Indian youths on reservations compared with a national sample of U.S. adolescents. JAMA Netw Open. 2018; 1: e180382.
- Stanley LR, Swaim RC. Initiation of alcohol, marijuana, and inhalant use by American Indian and White youth living on or near reservations. Drug Alcohol Depend. 2015; 155: 90-96.
- Whitesell NR, Mitchell CM, Spicer P, The Voices of Indian Teens Project Team. A longitudinal study of self-esteem, cultural identity, and academic success among American Indian adolescents. Cult Divers Ethn Minor Psychol. 2009; 15: 38-50.
- LaFromboise TD, Hoyt DR, Oliver L, Whitbeck LB. Family, community, and school influences on resilience among American Indian adolescents in the upper Midwest. J Community Psychol. 2006; 34: 193-209.
- Swaim RC, Stanley LR. Self-esteem, cultural identification, and substance use among American Indian youth. J Community Psychol. 2019; 47: 1700-1713.
- Swann WB, Chang-Schneider C, McClarty KL. Do people’s self-views matter? Self-concept and self-esteem in everyday life. Am Psychol. 2007; 62: 84-94.
- Swaim RC, Wayman JC. Multidimensional self-esteem and alcohol use among Mexican American and White Non-Latino adolescents: Concurrent and prospective effects. Am J Orthopsychiatry. 2004; 74: 559-570.
- Schick MR, Nalven T, Spillane N. The factor structure of self-esteem and its association with alcohol use in American Indian adolescents. Am J Orthopsychiatry. 2020; 90: 712-719.
- Rusby JC, Light JM, Crowley R, Westling E. Influence of parent–youth relationship, parental monitoring, and parent substance use on adolescent substance use onset. J Fam Psychol. 2018; 32: 310-320.
- Van Ryzin MJ, Fosco GM, Dishion TJ. Family and peer predictors of substance use from early adolescence to early adulthood: An 11-year prospective analysis. Addict Behav. 2012; 37: 1314-1324.
- Yap MBH, Cheong TWK, Zaravinos-Tsakos F, Lubman D, Jorm AF. Modifiable parenting factors associated with adolescent alcohol misuse: A systematic review and meta-analysis of longitudinal studies. Addiction. 2017; 112: 1142-1162.
- Patel H, Chambers R, Littlepage S, Rosenstock S, Richards J, Lee A, et al.The association of parental monitoring and parental communication with sexual and substance use risk behaviors among Native Americanyouth. Child Youth Serv Rev. 2021; 129: 106161.
- Krauss S, Orth U, Robins RW. Family environment and self-esteem development: A longitudinal study from age 10 to 16. J Pers Soc Psychol. 2020; 119: 457-478.
- Parker JS, Benson MJ. Parent-adolescent relations and adolescent functioning: Self-esteem, substance abuse, and delinquency. Adolescence. 2004; 39: 519-530.
- Sterrett-Hong EM, Kincaid C, Hardaway CR, Adams M, MacFarlane M, Jones DJ. Individual and family-level correlates of socio-emotional functioning among African American youth from single-mother homes: A compensatory resilience model. J Fam Issues. 2020; 41: 1355-1384.
- Amato PR, Fowler F. Parenting practices, child adjustment, and family diversity. J Marriage Fam. 2004; 64: 703-716.
- Caldwell RM, Beutler LE, Ross SA, Silver NC. Brief report: An examination of the relationships between parental monitoring, self- esteem and delinquency among Mexican American male adolescents. J Adolesc. 2006; 29: 459-464.
- deVries SLA, Hoeve M, Stams GJJM, Asscher JJ. Adolescent-parent attachment and externalizing behavior: The mediating role of individual and social factors. J Abnorm Child Psychol. 2016; 44: 283- 294.
- Wouters S, Colpin H, Luyckx K, Verschueren K. Explaining the relationship between parenting and internalizing symptoms: The role of self-esteem level and contingency. J Child Fam Stud. 2018; 27: 3403-3412.
- Özdemir Y, Vazsonyi AT, Çok F. Parenting processes, self-esteem, and aggression: A mediation model. Europ J Develop Psychol. 2017; 14: 509-532.
- Hunter SB, Barber BK, Stolz HE. Extending knowledge of parents’ role in adolescent development: The mediating effect of self-esteem. J Child Fam Stud. 2015; 24: 2474-2484.
- Swaim RC, Stanley LR. Psychometric evaluation of the Parental Monitoring Short Scale (PMSS). J Health Promotion Prev. 2023; 6: 70-93.
- Stattin H, Kerr M. Parental monitoring: A reinterpretation. Child Dev.2000; 71: 1072-1085.
- Swaim RC, Oetting ER, Edwards RW, Beauvais F. Links from emotional distress to adolescent drug use: A path model. J Consult Clin Psychol. 1989; 57: 227-231.
- Winer ES, Cervone D, Bryant J, McKinney C, Liu RT, Nadorff MR. Distinguishing mediational models and analyses in clinical psychology: Atemporal associations do not imply causation. J Clin Psychol. 2016; 72: 947-955.
- Muthén LK, Muthén BO. Mplus User’s Guide. Eighth Edition, 1998-2017.
- Yuan Y, MacKinnon DP. Bayesian mediation analysis. PsycholMethods. 2009; 14: 301-322.
- Asparouhov T, Muthén BO. Exploratory structural equation modeling.Struct Equ Mod. 2009; 16: 397-438.
- Boyd-Ball AJ, Vérroneau MH, Dishion TJ, Kavanagh K. Monitoring and peer influences as predictors of increases in alcohol use among American Indian youth. Prev Sci. 2014; 15: 526-535.
- Swaim RC, Stanley LR. Multivariate family factors in lifetime and current marijuana use among American Indian and White adolescents residing on or near reservations. Drug Alc Depend. 2016; 169: 92- 100.
- Jones RT, Kephart C, Langley AK, Parker MN, Shenoy U, Weeks C. Cultural and ethnic diversity issues in clinical child psychology. Handbook Clinic Child Psychol. 2001; 955-973.
- Rosenberg M. Conceiving the Self. New York: Basic Books. 1979.
- Haney P, Durlak JA. Changing self-esteem in children and adolescents: A meta-analysis review. J Clin Child Psychol. 1998; 27: 423-433.









































































































































{kind=link}