Diagnostic Dilemmas in Intraoperative Diagnosis of Glial Neoplasms
- 1. Department of Pathology, MVJ Medical College and Research Hospital, India
- 2. Department of Pathology, SDM College Medical Sciences and Hospital, India
ABSTRACT
Background: Intraoperative cytology is supportive and diagnostic of glial lesions. This is due to the dyscohesive nature of glial lesions and lack of dense connective tissue. We have tried to assess the utility of smear technique in rapid diagnosis of glial lesions.
Aims: To study the cytological features of various glial lesions and to assess the utility of smear technique in intraoperative diagnosis of these lesions by comparing the cytology features with their respective histopathologic features.
Setting & design: This study was conducted in the Department of Pathology, SDMCMSH, Dharwad over a period of 2 years.
Materials & methods: Twenty neurological specimens of suspected glial tumours received in the department of pathology for frozen section were studied. Squash preparation was done on all the cases and stained with Hematoxylin & Eosin (H & E) staining. An intraoperative diagnosis was made on squash preparation and frozen section slides. The diagnosis on squash smears was compared with the final diagnosis.
Results: Cytological correlation was seen in 18 out of 20 cases. Erroneous intraoperative diagnosis was given in one case each of oligodendroglioma and high grade astrocytoma. Hundred percent diagnostic accuracy of squash cytology was observed in cases of low grade astrocytomas, ependymoma, subependymoma and ganglioglioma.
Conclusion: Intraoperative cytology is fairly accurate and useful in intraoperative consultation of glial tumours. However squash technique has its limitations in certain cases like oligodendroglioma and grading of glial tumours.
KEYWORDS
Intraoperative cytology;Glial lesions;Squash cytology.
CITATION
Krishnappa I, Myageri A, Shastri DU, Rao R (2017) Diagnostic Dilemmas in Intraoperative Diagnosis of Glial Neoplasms. J Cancer Biol Res 5(1): 1092
INTRODUCTION
Primary CNS neoplasms are relatively rare, when compared to other malignant tumours. The annual incidence of CNS tumours ranges from 10-17 per 1,00,000 persons for intracranial tumour and 1 to 2 per 1,00,000 persons for intraspinal tumours [1].
Intraoperative consultation provides preliminary diagnosis and thus aids the neurosurgeon in subsequent surgical approach. It can guarantee that the surgeon is in the desired anatomic location and also ensures that adequate amount of abnormal tissue is available to the pathologist to render a final diagnosis on permanent sections [2]. Intraoperative frozen section diagnosis is asked for by the neurosurgeon mostly in cases of dilemma regarding the diagnosis being neoplastic or infectious. If there is an infectious process, an additional sample has to be sent for microbiological examination and also post-operative intensive antibiotic treatment needs to be started. In case of a neoplastic lesion, the type of neoplasm, as to that amenable to thorough surgical resection only or those requiring additional chemotherapy and radiotherapy as well, can be determined besides proving if the tumour is a primary or metastases from a distant site [3].
Intraoperative cytology techniques are particularly useful in discohesive lesions like abscesses, tumours such as gliomas, adenomas, lymphomas and some metastatic carcinomas. Therefore a comparative analysis is being done between squash preparation and regular histopathological examination in diagnosis of glial lesions, with an aim to identify the advantages and limitations of using squash studies along with frozen sections for intraoperative diagnosis.
AIMS AND OBJECTIVES
To study the cytological features of various glial neoplasms. To compare squash smear technique with histopathological examination (HPE) in diagnosis of glial neoplasms and to evaluate its usefulness.
MATERIALS AND METHODS
A prospective study of squash smears of glial lesions was carried out over a period of 2 years. Neurological specimens received in the department of pathology for frozen section were studied. Ethical clearance for conducting this study was obtained from the institutional ethical clearance committee. Specimens received in fresh state only were considered for the study and those sent in formalin fixative were excluded.
Preoperatively, clinical details of the patient like age, sex, symptoms and signs on presentation, clinical diagnosis along with other relevant clinical and radiological findings were noted. Tissue sent for intraoperative consultation was used for squash preparation that is, one to two millimetres of tissue was crushed between two slides in order to spread the tissue into a thin film, fixed in 95% alcohol and stained by H & E. Cytomorphological findings were observed on squash preparation. Frozen section slides were prepared by cutting the tissue on a cryostat apparatus and staining with haematoxylin-eosin stain. Intraoperative diagnosis was given based on the findings observed in the squash smears as well as the frozen section slides. Remaining tissue was processed routinely to produce paraffin embedded sections. These were observed and reported by another pathologist, who was blinded to the intraoperative diagnosis. Later on, the findings observed on cytology smears were compared with those present in the paraffin embedded sections. Comparing the initial intraoperative cytology and final histopathology diagnoses, established the diagnostic utility of squash cytology in diagnosing glial lesions.
RESULTS
Squash smears from 20 cases of clinically suspected glial neoplasms were analyzed. Figure (1)
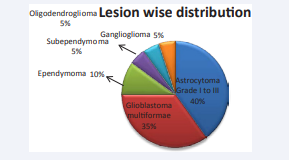
Figure 1 Lesion wise distribution of cases.
shows the distribution of cases based on the final histopathology diagnosis.
Maximum number of cases (8 cases, 40%) was astrocytoma grade I-III. One case of pilocytic astrocytoma was reported in an 8 year old male patient, which showed elongated piloid processes and Rosenthal fibres in the squash smears (Figure 2).
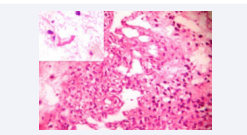
Figure 2 Pilocytic astrocytoma. Tumour showing microcystic areas and cells with piloid processes. Paraffin section H&E 10X. Inset – Squash smear, Rosenthal fibre. H&E 40X.
Five cases of diffuse fibrillary astrocytomas were reported which showed highly cellular smears with pleomorphic astrocytes on smears.
Second most common glial neoplasm in the present study (7 cases, 35%) was glioblastoma multiformae. Oldest patient was 72 years old and youngest patient was a 25 year old female. On MRI, 2 cases were reported as aggressive meningiomas, 2 cases as metastases and the others as gliomas. Squash smears showed increased cellularity, nuclear pleomorphism, and numerous atypical mitotic figures in a necrotic background. Paraffin embedded sections also showed similar features along with vascular endothelial proliferation. One case (5%) of subependymoma was reported. CT scan was reported as space occupying lesion in corpus callosum. Squash smears showed dense glial tissue having either patches of high cellularity and paucicellular fields with few cells. Since scant tissue was sent for intraoperative consultation no representative tissue could be seen in the frozen section. Diagnosis was give One case (5%) of ganglioglioma was reported which on squash smears showed large ganglion cells with round nucleus, prominent large nucleoli and moderate to abundant granular cytoplasm, along with neoplastic astrocytes (Figure 3A).
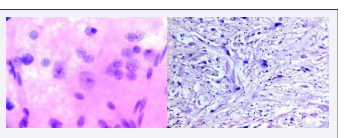
Figure 3 Ganglioglioma. A, Ganglion cells in the midst of neoplastic astrocytes. Squash smear H&E 40X. B, Dysplastic ganglion cells with neoplastic astrocytic element. Paraffin section H&E 10X.
Histopathology sections also showed neoplastic astrocytes and large dysplastic ganglion cells (Figure 3B)
Two cases (10%) of ependymomas were reported in the present study. Squash smears showed monomorphic cells forming perivascular pseudorosettes along with occasional true rosettes (Figure 4A).
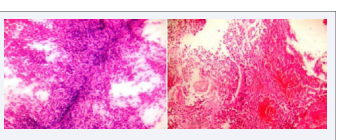
Figure 4 Ependymoma. A, Monomorphic cells forming perivascular pseudorosettes. Squash smear. H&E 4X. B, Tumour cells forming ependymal canal and perivascular pseudorosette. Paraffin section. H&E 4X.
Permanent sections showed monomorphic cells forming ependymal canals and perivascular pseudorosettes (Figure 4B).
Among the 8 cases of astrocytomas (Grade I-III), 7 cases correlated cytologically (87.5%). One case of oligodendroglioma was misdiagnosed as astrocytoma on cytology (Figure 5A,B).
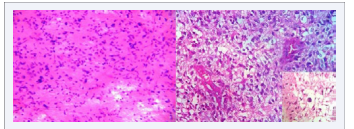
Figure 5 Oligodendroglioma. A, Highly cellular smear, pleomorphic glial cells. Squash smear H&E 10X. B, Neoplastic oligodendroglial cells surrounded by a clear halo, thin walled blood vessels (chicken wire pattern), Inset - Calcification. Paraffin section H&E 40X.
It was reported as space occupying lesion (SOL) in left frontal cortex in magnetic resonance imaging (MRI). Among the 7 cases of GBM, 6 cases (85.71%) were diagnosed correctly on cytology; one case which was given as right temporal SOL on MRI, was reported as Astrocytoma grade III on intraoperative cytology (Figure 6A,B).
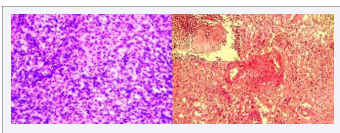
Figure 6 Glioblastoma multiformae. A, Increased cellularity with occasional mitosis and vascular proliferation. Squash smear H&E 10X. B, Endothelial proliferation, pleomorphic tumour cells in sheets. Inset – necrotic focus. Paraffin section H&E 10X.
One case which was reported as astrocytoma grade IV on cytology was later diagnosed as anaplastic medulloblastoma on permanent sections (Figure 7A,B).
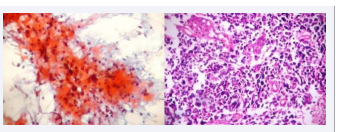
Figure 7 Anaplastic medulloblastoma.A. Highly pleomorphic cells in fibrillary and necrotic background. Squash smear Pap stain 10X. B, Anaplastic medulloblastoma. Pleomorphic tumours cells and occasional giant cells. Paraffin section H&E 10X.
However since this study includes only glial neoplasms, this case of anaplastic medulloblastoma has not been included for analysis.
Accuracy rates of intraoperative cytology for the various lesions observed in our study are shown in Table (1).
|
Table 1: Accuracy rates of squash cytology in diagnosis of individual lesions. |
||||
|
Sla No |
Lesion |
Final diagnosis |
Cytology correlation |
Accuracy % |
|
1 |
Astrocytoma (Grade I-III) |
8 |
7 |
87.5 |
|
2 |
Glioblastoma multiformae |
7 |
6 |
85.71 |
|
3 |
Ependymoma |
2 |
2 |
100 |
|
4 |
Subependymoma |
1 |
1 |
100 |
|
5 |
Ganglioglioma |
1 |
1 |
100 |
|
6 |
Oligodendroglioma |
1 |
0 |
0 |
DISCUSSION
Eisenhardt and Cushing in early 1930’s initiated the technique of intraoperative cytology which was further documented by Russel et al., in 1937. The present technique was introduced by her along with Sir Hugh Cairns in 1930’s [4].
Brain being a delicate organ with numerous vital centres and essentially no regenerative activity, obtaining generous material intraoperatively is difficult. Therefore most of the times diagnosis has to be made on limited tissue submitted by the neurosurgeon [5]. Thus arises the need for cytology techniques to arrive at a diagnosis intraopearatively. Various techniques used for rapid examination of biopsy material for intraoperative diagnosis are, touch preparation, crush preparation and squash smear technique.
Disadvantage of touch method is that smears cannot be made properly from small specimens which require handling the tissue with forceps, brain tissue being extremely soft can get distorted by excessive handling. Crush smears usually leave a big glob of tissue in centre of slide which is too thick to be useful under microscope. These drawbacks can be overcome by using the smear technique for intraoperative diagnosis of CNS lesions. The variable thickness of the smear offers an advantage. In the peripheral thin portion the cytological details of the whole cell can be visualized, while the central thick portion provides the general architectural detail especially the tumour cell relation with the vessel and the vascular changes [1]. The advantage of cytology over frozen sections for intraoperative consultation is that cytology helps to evaluate wider areas, which is crucial in glial lesions as different areas might show different grade. Further it is easier to obtain good cytology smears rather than frozen sections in brain lesions. A good cytological preparation of brain displays high cellularity, crisp nuclear and cytoplasmic details, and occasionally the tissue architecture. Whereas frozen sections on brain tissue may develop many artefacts like ice crystal artefact and water logging in tissues. Thus making the sections look smudgy, foggy and shattered [6]
In our study, the most commonly seen glial neoplasm was astrocytoma Grade I to III, similar to other studies as elaborated in Table (2).
|
Table 2: Comparision of incidences of glial neoplasms. |
|||||||
|
Lesion |
Roessler K et al [7]
|
Kini J R et al [8]
|
Iqbal M et al [9]
|
Ghoshal N et al [10]
|
Shukla K et al [11]
|
Khamechian T et al [12]
|
Present study |
|
Astrocytoma |
487
|
14
|
7
|
45
|
140
|
48
|
8
|
|
GBM |
616
|
17
|
10
|
28
|
- |
6
|
7
|
|
Ependymoma |
76
|
2
|
16
|
13
|
18
|
- |
2 |
|
Subependymoma |
- |
- |
- |
- |
- |
- |
1 |
|
Ganglioglioma |
- |
- |
- |
4
|
- |
- |
1 |
|
Oligodendroglioma |
68
|
9
|
13
|
20
|
- |
6
|
1 |
However present study shows lesions like subependymoma and ganglioglioma which were not reported in other studies.
The diagnostic accuracy of smear technique in our study was hundred percent for ependymoma, subependymoma and ganglioglioma. It was slightly lesser for astrocytomas and glioblastoma multiformae. These findings were in comparison with other studies as shown in Table (3).
|
Table 3: Comparision of accuracy rates of squash cytology in diagnosis of glial neoplasms with other studies. |
||||||
|
Lesions |
Roessler K et al [7] |
Kini J R et al [8] |
Shukla K et al [11] |
Khamechian T et al [12] |
Nigam S K et al [13] |
Present study |
|
Astrocytoma |
96.7% |
100% |
96.42% |
81% |
84% |
87.5% |
|
GBM |
95.7% |
64.7% |
- |
66% |
84.6% |
85.71% |
|
Ependymoma |
77.6% |
100% |
83.33% |
- |
50% |
100% |
|
Subependymoma |
- |
- |
- |
- |
- |
100% |
|
Ganglioglioma |
- |
- |
- |
- |
- |
100% |
|
Oligodendroglioma |
80.9% |
22.2% |
90% |
100% |
33.3% |
0 |
In the present study one case of oligodendroglioma was misdiagnosed as astrocytoma on squash smears. Such discrepancy has been reported in other studies as well like the ones done by Kini J R et al., (22.2%) and Nigam S K et al., (33.3%) [8,13]. Oligodendrogliomas on cytology show uniform round cells in a fibrillary background with thin blood vessels and occasional calcification [14].Oligodendroglial tumour nuclei appear round and uniformly hyperchromatic; however, freezing tissue often produces irregularities in the nuclear contours of an oligodendroglioma, making it look similar to an astrocytoma [15].Definitive differentiation of astrocytic and oligodendroglial elements is possible mostly on paraffin embedded sections only, as prompt fixation is responsible for the perinuclear halo in oligodendrocytes, which is a characteristic feature of oligodendrogliomas. However few authors have reported a higher accuracy of squash cytology in diagnosing oligodendrogliomas namely Roessler K et al., (80.9%), Shukla K et al., (90%) and Khamechian T et al., (100%) [7,11,12]. The accuracy rates for diagnosing oligodendrogliomas on cytology can be increased by correlating clinical and radiological details along with a keen observation of cytology smears.
In the present study, diagnostic accuracy of cytology in diagnosing glioblastoma multiformae (GBM) was 85.71%. This is similar to the diagnostic accuracy seen in studies carried out by Roessler K et al., (95.7%) and Nigam S K et al., (84.6%) [7,13]. One of the cases was reported as grade III astrocytoma on cytology, which turned out to be GBM on permanent sections. This was due to the absence of necrosis in the squash smears and frozen sections. Many authors are of the opinion that it is unwise to grade and subclassify gliomas on intraoperative consultation. Low grade astrocytomas like pilocytic astrocytomas may be overgraded due to increased vascularity and nuclear atypia. Freezing artifacts further increase the difficulties encountered [16]. Therefore one should avoid a vigorous attempt of grading these lesions on cytology. Morigaurd et al., suggested multiple biopsies from different areas to decrease the rate of false positivity and false negativity [14].
Another commonly encountered difficulty in intraoperative diagnosis of glial neoplasms is differentiation between low grade astrocytomas and reactive gliosis. Microscopically hypercellularity observed in gliosis is evenly distributed with predominance of astrocytic cells having eccentric bland nucleus, many long dendritic processes, with mild nuclear irregularity, low nuclear cytoplasmic ratio and delicate chromatin. Occasional binucleate cells can be encountered [17]. This type of gliotic smears may be seen in periphery of any CNS lesions like metastatic carcinoma, Craniopharyngioma, brain abscess etc. Thus making it desirable to ask the neurosurgeon to send a new and larger specimen in case of clinical deference. In contrast, tumor cells found in low grade fibrillary astrocytomas have increased nuclear-cytoplasmic ratios with little discernible cytoplasm. Astrocytoma nuclei have markedly irregular contours with hyperchromasia and unevenly distributed chromatin [1]. Reviewing the radiological data prior to arriving at a diagnosis intraoperatvely is a must as glial neoplasms present as space occupying lesions unlike reactive gliosis.
Ultimately the goal of a pathologist in intraoperative setting is not to diagnose and grade every case definitively but to provide sufficient preliminary information to optimize the surgery, as intraoperative cytology has its own limitations in diagnosing CNS lesions. Most of the errors in intraoperative reporting occur when the pathologist succumbs to pressure from the operating surgeon and also due to misleading clinical and radiological data. Besides, the volume of tissue sent for intraoperative consultation is sometimes scanty and not representative. Good correlation of clinical, radiological and microscopic features is required for a precise diagnosis.
CONCLUSION
Recent advance in CT scan aided biopsies suggests that in future we will see many small biopsies where smear technique will have to be used for diagnosing a lesion intraoperatively. The ability to remove a small bit of tissue and to ascertain whether or not the biopsy is positive or negative for malignancy in a stipulated period of time represents an undoubted advantage of smear technique over frozen section method. Familiarity with lesions and experience of the reporting pathologist in diagnosing neural lesions are important factors, which could improve the diagnostic accuracy of squash cytology. Undergrading of some glial neoplasms may occur due to inadequate tumoural sampling. Some oligodendroglial neoplasms might be misdiagnosed as astrocytomas, however immediate management does not change as both are low grade tumours. Squash preparation and frozen section are procedures that complement each other and assist the pathologist in offering a useful diagnosis. Therefore it would be ideal to do both the procedures in neurosurgical intraoperative consultation.








































































































































