Primary Squamous Cell Carcinoma of the Thyroid
- 1. Medical student, The Commonwealth Medical College, USA
- 2. Cancer Treatment Center at Hazleton, USA
ABSTRACT
Primary squamous cell carcinoma of the thyroid represents less than 1% of all thyroid malignancies. Unlike other thyroid cancers, it is often fatal. We report a rare case of a male patient with primary squamous cell carcinoma of the thyroid. This paper emphasizes the importance of fine needle aspiration in diagnosis, the urgency of early diagnosis and the importance of multi-modality treatment.
KEYWORDS
Thyroid ; Cancer ; Squamous Cell Carcinoma.
CITATION
Kuczmarska A, Patel MD, Mehta N (2014) Primary Squamous Cell Carcinoma of the Thyroid. J Cancer Biol Res 2(2): 1051.
ABBREVIATIONS
SCC: Squamous Cell Carcinoma.
INTRODUCTION
Thyroid cancer is the most common endocrine malignancy [1] and is the seventh most common cancer in women. [2] Typically, these malignancies are of papillary, follicular, or medullary histology, arising from normal tissues present in the thyroid. Patients will rarely manifest with primary squamous cell carcinoma of the thyroid even though the thyroid lacks squamous cell epithelium. Though this puzzling pathology accounts for less than 1% of thyroid malignancies, [3] it has an unusually high mortality making early diagnosis and treatment crucial for patient survival. We report a case of a male patient with primary squamous cell carcinoma of the thyroid and discuss the diagnosis, workup, epidemiology, treatment, and postulate etiologies of these unusual cancers.
CASE PRESENTATION
A 66 year old male presented with progressive loss of voice for one month in duration. The patient was otherwise asymptomatic. His past medical history is significant for hypertension controlled by medication and is negative for prior radiation or chemotherapy. His social history is significant for a 20 year smoking history, but cessation occurred 29 years ago. Family history is negative for malignancy and he denies recent weight loss.
Ultrasound guided fine needle aspiration cytology of the right thyroid showed a squamous lesion with atypia. Neck CT showed a low-density mass involving the posterior inferior right side of the thyroid gland extending posteriorly and medially to the tracheoesophageal groove. PET-CT showed a hypermetabolic lesion associated with the posterior right thyroid lobe with no regional or distant metastatic disease (Figure 1).
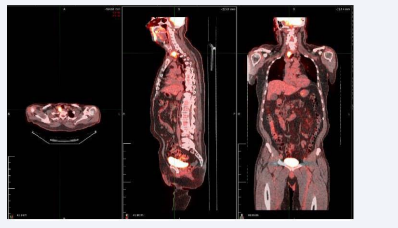
Figure 1 PET-CT demonstrating increased uptake in the posterior aspect of the right lobe of the thyroid with no distant metastatic disease
Esophagogastroduodenoscopy and rigid direct laryngoscopy showed right true vocal cord paralysis due to recurrent laryngeal nerve involvement.
The patient underwent right thyroidectomy with a right sided selective lymphadenectomy. Pathology showed a 2 cm well-differentiated stage IVa T4aN0M0 squamous cell carcinoma invading into the surrounding adipose tissue and skeletal muscle. Gross residual disease was present post-operatively. There were four negative lymph nodes. Subsequently, the patient had 2 cycles of high dose cisplatin and underwent external beam radiation therapy to decrease the risk of local recurrence with a dose of 6,300 cGy over six treatments (Figure 2, Figure 3).
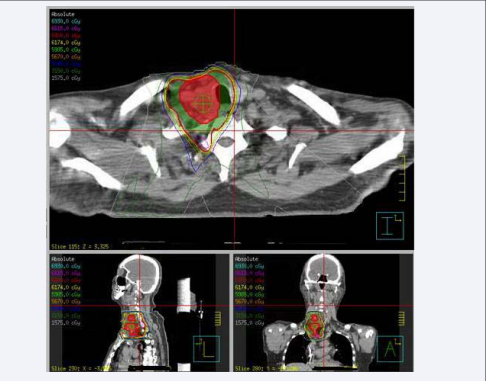
Figure 2 Radiation treatment plan for patient with right squamous cell carcinoma of the thyroid. The PTV is delineated in red and received 3700 cGy in 35 fractions. Avoidance structures included the left and right parotid glands, spinal cord, cochlea, larynx, eyes, and brainstem. The 5985 cGy isodose line is shown in light green; the 5040 isodose line in purple.
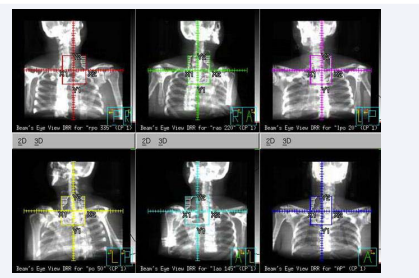
Figure 3 Beams Eye View of individual radiation beams used in the treatment of squamous cell carcinoma.
At follow-up, patient had mild induration but no mass effect in the neck. He also complained of some mild hoarseness, but reported decreased dysphagia. Physical exam showed no oral cavity thrush and no residual hyperpigmentation of the neck. Near treatment end, the last cycle of chemotherapy was held due to neutropenia. Roughly 11 months after symptoms first presented, the patient is still alive and repeat PET scan demonstrated no recurrent mass or residual disease and no regional or distant metastatic disease.
DISCUSSION
Primary squamous cell carcinoma of the thyroid is a rare tumor that accounts for less than 1% of all thyroid malignancies, [3] with 10 cases identified in a 25 year period (1978-2003). [4] This cancer typically affects older patients in the fifth and sixth decades of life, [3] with a mean age of 63 years and with a 2:1 female predominance. [5]
At diagnosis, primary SCC is typically found invading the trachea, esophagus, and other surrounding structures. [6] At presentation, patients will most commonly complain of an anterior neck mass, dyspnea and dysphasia. [5] Diagnosis of SCC of the thyroid is typically through fine needle aspiration, [7] although a distinction between primary SCC of the thyroid and a secondary metastatic SCC cannot be made. Further investigation via PET-CT is necessary to make a further distinction. Immunohistochemistry of SCC demonstrates positive staining of p53, p63, cytokeratins 7-19, and squamous cell carcinoma antigen, in addition to negative staining for thyroid transcription factor (TTF) and calcitonin. [8-10]
Mean survival time for patients with SCC of the thyroid is 9 months, with a 20% 3-year survival rate. [5] In comparison, the mean survival rate of patients with metastatic papillary carcinoma, the most common thyroid malignancy, is significantly higher at 76.6%. [11] The cause of death in the majority of SCC of the thyroid is airway compromise. [4]
There is currently no standard of care for treatment for primary SCC. Due to the aggressive nature of the disease, total thyroidectomy alone has led to minimal survival time. [12,13] Some studies have shown that patients have achieved greater longevity using aggressive regional surgery and post-operative radiotherapy, with reported survival up to 31 months. [14,15] However, no prospective trials have directly compared longevity using combination therapy versus thyroidectomy alone. In the present case, although the patient had gross residual disease post-operatively, he has exceeded the mean survival time with post-operative treatment consisting of high dose Cisplatin and radiation therapy with no residual or metastatic disease according to his latest PET-CT scan. This suggests that using a combination of Cisplatin-based chemotherapy, radiation and surgery would prolong patient survival, not unlike the data in the treatment of other cancers.
While the etiology of SCC of the thyroid remains uncertain, three theories have been postulated to explain the pathogenesis of this condition. The embryonic nest theory suggests that embryologic remnants, such as the thyroglossal duct, give rise to epithelial cells, [16] while the de-differentiation theory suggests that existing thyroid carcinoma of papillary, follicular, or medullary histology de -differentiates into SCC. [17] Another theory called the metaplasia theory hypothesizes that local inflammatory condition, such as Hashimoto’s thyroiditis, results in squamous metaplasia. [18] In the present case, since the patient has no past medical history of chronic inflammatory conditions, the embryonic nest theory and de-differentiation theory are more likely.
SCC of the thyroid is a rare condition that is often diagnosed late in the disease process, leading to low survival rates. Since the condition is aggressive and fatal, it is important to recognize the associated symptoms sooner in both male and female patients. In the present case, the tumor was discovered late in stage IVa, but nevertheless, the cancer is in remission. Part of this success can likely be attributed to the multi-modality treatments, suggesting that a multi-modal approach can increase survival and prevent recurrence even in late stages. Observing and documenting more patients with this rare malignancy will continue to develop our understanding of the etiology, diagnosis, and treatment of the disease in order to best care for our patients.
CONFLICT OF INTEREST
We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us.
We understand that the Corresponding Author is the sole contact for the Editorial process. She is responsible for communicating with the other authors about progress, submissions of revisions and final approval of proofs.







































































































































{kind=link}