Sugar Coating of the Cerebellum
- 1. British Columbia Cancer Agency, Division of Medical Oncology, Vancouver BC, Canada
CITATION
Metcalf C, Villa D (2013) Sugar Coating of the Cerebellum. J Cancer Biol Res 1(2): 1010
CLINICAL IMAGE
A 54-year-old premenopausal woman underwent left mastectomy and sentinel lymph node biopsy for extensive ductal carcinoma in-situ with microinvasive estrogen receptor negative and HER2 overexpressing breast cancer, without nodal involvement. She did not receive adjuvant systemic or radiation therapy. She presented two years later with severe cerebellar ataxia, diplopia, blurred vision, nausea, and headache. Computed tomography scan showed abnormal left axillary and retropectoral lymph nodes as well as a small sclerotic lesion in the L3 vertebra. Biopsy of a left axillary lymph node was significant for estrogen receptor negative and HER2 positive invasive ductal carcinoma.
Magnetic resonance imaging (MRI) of the brain showed focal cortical enhancement in the lateral right cerebellar hemisphere. There was thin irregular enhancement throughout the leptomeningeal spaces of the posterior fossa, notably along the cerebellar fissures and outlining the brain stem, with a ”sugar coating” or Zuckerguss pattern (Figures 1 and 2, white arrows).
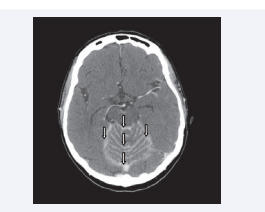
Figure 1 Axial image of the gadolinium-enhanced MRI showing enhancement throughout the leptomeningeal spaces of the posterior fossa, highlighting the Zuckerguss pattern around the cerebellum and brain stem (white arrows).
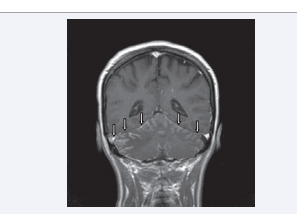
Figure 2 Coronal image of the gadolinium-enhanced MRI showing enhancement throughout the leptomeningeal spaces of the posterior fossa, highlighting the Zuckerguss pattern around the cerebellum (white arrows).
Cerebrospinal fluid (CSF) cytology revealed malignant cells consistent with adenocarcinoma. With a diagnosis of leptomeningeal carcinomatosis, she was managed with systemic high-dose methotrexate with transient neurologic improvement, but deteriorated and died three months later.
Leptomeningeal carcinomatosis is most commonly seen in breast carcinoma, lung carcinoma, and melanoma. The identification of malignant cells in the CSF constitutes the gold standard for diagnosis. However, the sensitivity of a single CSF analysis is approximately 50%. Gadolinium-ehnanced MRI is the imaging modality of choice, with sensitivity as high as 90%, even with a negative CSF cytology [1]. On the other hand, the false negative rate of MRI is about 60%, which reinforces the role of CSF analysis in patients with clinical suspicion for leptomeningeal metastases with normal brain MRI [2]. The Zuckerguss pattern is not specific for any particular tumor type; therefore, histologic evidence of metastatic malignancy is required to make a diagnosis and select therapy. National Comprehensive Cancer Network guidelines support the use of MRI alone to establish a diagnosis if radiologic findings are consistent in the setting of supportive clinical signs and symptoms [3].







































































































































{kind=link}