The Remadi’s technique or the Bentall Technic? Valsalvas Reduction Plast
- 1. Cardio-vascular surgery unit, Amiens South Hospital, France
- 2. Cardiology unit, Amiens South Hospital, France
Abstract
The objective of this study was to find an another surgical way than Bentall procedure to treat the aneurysms of ascending aorta involving the sinuses of valsalvas.
From September 2008 to May 2018, eighty five patients underwent aortic valve replacement (AVR) associated with a Valsalva plasty, with or without the replacement of the ascending aorta. All the procedures were performed by a single surgeon (Remadi’s technique) at Amiens Universitary Hospital in France.
There was no operative death. During the follow-up at ten years, the diameters of the Sinuses of Valsalva remain steady, without long term post-operative aneurysm or reoperation for any aortic complication. This original new technic, can be applied safety for almost all ascending aorta aneurysms involving valsalvas (more than 90% of cases) instead of the bentall procedure.
This new technic is safe with excellent immediate and mid- term results. The Remadi’s technic is particularly adapted for the older patients or patients with associated comorbidity in order to reduce the operative risk. The Bentall’technic should be performed only when the ascending aorta has a shape like a « chianti bottle with very important dilatation of sinuses of valsalvas, when its the only procedure adapted for those remaining indications.
Keywords
• Surgery
• Aneurysm
• Valsalvas
CITATION
Remadi JP, Szymanski C. The Remadi’s technique or the Bentall Technic? Valsalvas Reduction Plasty. J Cardiol Clin Res. 2023; 11(2): 1194.
INTRODUCTION
The gold standard treatment of aortic root pathology with associated aortic valve disease and dilatation at sinuses of valsalvas has been the Bentall procedure for forty years. The Bentall procedure was first described by Hugh Bentall and Antony De Bono in 1969 [1]. This procedure is performed with a composite valved graft, either mechanical or biological, in order to replace the entire aortic root and valve with the reimplantation of the coronary arteries associated to a whole resection of the three Valsalva sinuses to avoid secondary excessive dilatation with a risk of rupture or aortic dissection.
The Bentall operation has demonstrated good midteerm and long-term survival however. A potential shortcoming of this procedure is the risk of valve-related events: particularly structural deterioration for biologic valves, bleeding and thromboembolism for mechanical valves. The coronary ostia stenosis could encountered ischemic event and sudden death. Ostia aneurysms are also a major issues of the Bentall procedures.
The present prospective study was performed to assess outcomes in a series of consecutive patients from a single institution, who underwent « A Valsalva plasty » procedure (Remadi’s technic) for a variety of aortic root diseases, to study whether we could define a subset of patients comparable to those who might currently be considered for traditional and historical Bentall procedures.
PATIENTS AND METHOD
From September 2008 to May 2018, eighty five patients underwent aortic valve replacement (AVR) with a « Valsalva plasty » associated with an ascending aorta replacement by a single surgeon (Remadi’s technique) at Amiens Hospital in France (Figure 1,2). The study was approved by the local ethics committee without requiring individual patient consent. Among the eighty five patients 78 LPI graft prosthesis and 4 Joteck prosthesis were implanted. Three patients underwent only an AVR with a valsalva plasty. Sixty bioprostheses and 25 mechanical prostheses were implanted. Mean age was 63.5 ± 15 years and sex ratio was 2.7 (62 male/23 female) (Table 1). All patients were operated on through a full sternotomy within a standard cardio-pulmonary bypass under normothermia, and anterograde cardioplegia was systematically used. A « plasty-reduction » of dilated sinuses of Valsalva (Figure 1), was performed in all cases. The excess tissue was excluded and secured during the prosthesis implantation. A continuous suture of polypropylene 2/0 sewed the annulus with the folds of the Valsalvas. At the end of the procedure the coranary ostia were lowered in the right place if they were too high. Aortic clamp time was similar to the implantation of a standard prosthesis and avoided the manipulation of coronaries ostia. The dacron prosthesis was implanted in a supra coronary position replacing the ascending aorta. Ten patients having major comorbidity or severe heart failure underwent this technic with a shorter aortic cros clamp time. The mean aortic cross clamping and the CPB time respectively amounted to 48 ± 23 and 61 ±16 mn.
Follow-up and Statistics
All patients were discharged from hospital. Follow-up ended in December 2019. The follow-up was 100% complete. Mean follow-up time was 110 ± 7,9 months for a total of 9320 months. Eighty one patients were alive at the end of follow-up. CT scan was performed for each patient during the last 6 months of 2019.
STATISTICAL METHOD
Statistical analysis was performed with SPSS 22 (SPSS Inc., Chicago, IL). Continuous variables were expressed as mean ± standard deviation and compared using Student’s t test or Mann Whitney test where appropriate. Qualitative variables were expressed as a percentage and compared by χ2 test or Fischer’s exact test where appropriate. A p value less than 0.05 was considered statistically significant.
RESULTS
Surgical Outcome
A Complete « reduction-plasty » of sinuses of valsalvas « reduction-plasty » was performed for all patients (Figure 1,2).

Figure 1 Non coronary valsalva plasty.
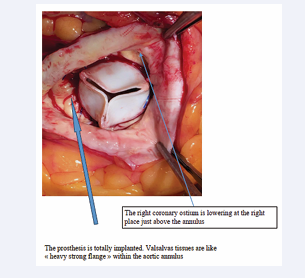
Figure 2: Prosthesis totally implanted with Valsavas plasty.
There was no Hospital death (at 30 days). One patient was reoperated on for post-operative major bleeding at H4. One patient had a transient stroke but fully recovered before hospital discharge. The atrial fibrillation (AF) was the most common post-operative complication (40%). All these AF were transient and furthermore there was no permanent AV block. The length of post-operative intensive care stay was 48 ± 23 hours. Mean hospital stay was 9.4 ±7 days and all patients were discharged from hospital.
There was four late deaths unrelated to the previous surgery. Three late death were due to a neoplasm and one death was related to an end renal failure. One patient was readmitted for a major bleeding due to an INR>7 without consequences. A CT scan of the thoraco-abdominal aorta was performed for all patients. There was two minor thrombo-embolism events, none valve thrombosis, reoperation, coronary event and one acute infective endocarditis during the follow-up. Two patients were reoperated on for a bioprosthesis structural détérioration.
The diameters of the Valsalva sinuses were steady without any secondary aneurysm (Table 2), or reoperation for aortic dissection or other complications.
DISCUSSION
Ascending aorta replacement with or without aortic valve replacement has become a standard surgical procedure. When a dilatation of the Valsalvas is associated, the Bentall procedure has been the gold standard for the last thirty years [1]. The resection of the sinuses of Valsalva has been accepted as the best choice in those cases. Numerous studies during the last twenty years have shown the good results of the Bentall procedure [2-6]. The diameters of the aorta, valsalvas and sinotubular junction have been studied to evaluate the good timing for surgery. Nevertheless, the Bentall procedure presents some well-known limitations and complications [7]. In a large Meta-analysis, Mookhoek et al., show that the operative mortality amounts to 6%. The operative mortality of AVR associated with supra coronary ascending aorta replacement is lower amounting to 2% [7]. So, the difference between the two technics in term of mortality is 3 time higher for the Bentall procedure. Furthermore, the follow-up is worse than expected with higher late mortality for the Bentall procedure [7]. The false aneurysms of the coronary ostia and the ischemic events are the worse complication of the Bentall technic.
First of all, the manipulation of the coronary ostia is not harmless and provides a longer surgery procedure with added risks. In another hand, when a biological Bentall failed, the redo procedure is more difficult than an isolated redo AVR, therefore the results are worse. Numerous studies proposed a revised Bentall procedure [8-12], but all those techniques include reimplantation of the coronary ostia which is the “Achille’s heel” of this procedure. Aortic valvular repair was proposed by David et al but had the same limitations about the coronary ostia reimplantation [13-15]. The aortic plasties described in the literature are completely different. Those technics of aortoplasty like subcommisural annuloplasty described by El Koury represent very difficult and longer procedures, and doesn’t involve the same indications.
The Remadi’s technic could replace the Bentall procedure for the main indications instead of the Bentall procedure (more than 90% of the cases). Therefore the Bentall procedure must be performed only when the sinuses of Valsalva present an huge dilation with a very high coronary ostia elevation: we can’t avoid this technic! This situation represents few cases of the ascending aorta dilatation. Most of the Bentall procedures are performed for moderate uniform dilatation(not the “Chianti bottle shape”) of the ascending aorta with a level of coroanary Ostia close to the normal and can be easily avoided with excellent results using the the Remadi’s technic.
The technique of Valsalva plasty-reduction (Remadi’s technic) make an easy exclusion of the fragile tissue. At the end of the procedure when the prosthesis is implanted, the coronary ostia are lowering about 0.5 to 1.5 cm. In some cases the three Valsalvas are dilated but in most cases only 2 or even 1 sinus are dilated.
This technique can be applied to ascending aorta replacement and aortic prosthesis replacement or only to AVR when only the sinuses of Valsalva are dilated without an ascending aorta dilatation. This technic is safe with excellent immediate and long term results. The coronary ostia are not manipulated and if a redo procedure is indicated during the follow-up for structural détérioration of a biological prosthesis, it’s « like an isolatedAVR redo procedure »
During the follow-up no secondary false aneurysm was observed, and the diameters were steady.
This procedure is particularly interesting for old patients or poor left ventricular function because the aortic cross clamping and CPB time are significantly shorter than for a Bentall procedure.
The continuous rolling suture is adapted to this technique to secure the valve with a simultaneous reduction of the Valsalva tissue. Secondary aneurysm of the coronary ostia known after Bentall procedure is due to the suture itself and to the remaining tissue [7,12-15]. When the « reduction plasty » of the sinuses of Valsalva is performed the remaining tissue is heavy, strong and secured, without the coronary ostium manipulation which can involve falses aneurysms or ostium twist leading to a secondary ischemia. Another superiority of the Remadi’s technic over the bentall procedure is provided for the redo and TAVI procedures. Because the redo procedure become like an isolated AVR reintervention and the coronary ostia are located in an anatomical place which is crucial for TAVI.
CONCLUSION
The Remadi’s Technic is adapted for numerous situations: one, two or three dilatation of sinus of valsalvas and can be performed rather than the Bentall procedure. This technic is easily reproductible safe and shorter than the Bentall procedure. This kind of valsalva plasty was never described and is a true useful innovation. The plasties of aortic annulus and aortic root described on the literature are totally different, and are procedures with longer CPB and aortic cross clamp time and doesn’t involve the same disease. The midterms results are excellent with no cases of reintervention of complication on the sinuses of valslvas. The shorter CPB and cross clamping time are very useful to lower the operative risk for elderly and fragile patients. The anatomical conservation of the coronaries ostia location is also very useful in the case of a secondary procedure like TAVI or a redo surgery. Using the continuous suture remains the key-point of this procedure.








































































































































{kind=link}