Spontaneous Renal Pelvis Rupture Caused by Ureteral Lithiasis
- 1. Universidade Estadual do Oeste do Paraná, Rua Universitária, Brasil
- 2. Thaís Figueiredo Teodoro de Oliveira, Faculdade Assis Gurgacz, Avenida das Torres, Brasil
ABSTRACT
Introduction: Rupture of the urinary collecting system associated with peripelvic extravasation of the urine is an extremely rare outcome of the increased pressure in the pelvis during renal colic.
Case report: We present a case of a 40-year-old woman with clinic of renal colic. No history of nephrolithiasis or surgical procedures. She was primarily treated with symptomatic medication in the emergency room. Imaging exams showed hydronephrosis grade II, abundant fluid collection in perinephric area, free passage of contrast material from the pelvis renalis to around the kidney and a calculi in left terminal ureter. She was referred to urology service and treated with placement double-J ureteric stent. Postoperatively with good development, asymptomatic. After 30 days, the double J catheter was removed and ureteroscopy performed without abnormalities.
Conclusion: Spontaneous rupture of the renal pelvis is a disease without characteristic clinical signs. The diagnosis can be suspected on ultrasonography, and confirmed by computed tomography using contrast. In ureteral stones expected to pass under observation or treated with medical expulsive treatment, the possibility of renal pelvis rupture should be kept in mind.
KEYWORDS
• Renal pelvis
• Rupture
• Ureteral lithiasis
• Renal colic
CITATION
Batista Peres LA, Leonel Ferreira JR, de Oliveira TFT (2015) Spontaneous Renal Pelvis Rupture Caused by Ureteral Lithiasis. J Clin Nephrol Res 2(2): 1025.
ABBREVIATIONS
CT: Computed Tomography
INTRODUCTION
Ureteral stones are 20% of urinary tract stones [1]. Most of stones located at distal ureter pass spontaneously under observation or medical expulsive treatment; however, some are complicated with urinary tract infection, hydronephrosis, and renal function disturbances [1,2].
Rupture of the urinary collecting system associated with peripelvic extravasation of the urine is a rare condition and commonly associated with obstructing calculus, trauma or previous urinary tract surgery [3,4]. Collecting system rupture is an extremely rare outcome of the increased pressure in the pelvis during renal colic. The diagnosis can be suspected on serial ultrasonography, and confirmed by contrast enhanced CT scan [3].
CASE PRESENTATION
A 40-year-old woman has been admitted to the emergency department with acute pain in the left flank, with characteristics of renal colic. No history of nephrolithiasis or surgical procedures. Physical examination: good general condition, eupneic, a febrile, facies of pain. Cardiac and pulmonary auscultations were normal. She had mild abdominal distension and pain on superficial and deep palpation in the left flank. Lower limbs hadn’t edema. Laboratory exams showed urine analysis exhibiting haematuria and creatinine 0.9 milligrams mg/dL.
She received symptomatic treatment in hospital. In urinary ultrasonography, hydronephrosis grade II and abundant fluid collection in perinephric area was seen. The abdominal computed tomography (CT) confirmed the finding (Figure 1).

Figure 1 Abdominal CT. Abundant fluid collection in perinephric area and hydronephrosis grade II.
The delayed phase of the contrast enhanced CT scan showed free passage of contrast material from therenal pelvis to around the kidney (Figure 2)

Figure 2 Abdominal CT with contrast enhanced. Free passage of contrast material from the left renal pelvis to around the kidney and spontaneous rupture of the renal pelvis.
and a calculi in terminal ureter (Figure 3).
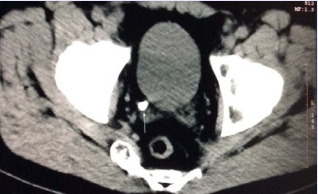
Figure 3 Abdominal CT. Calculi in left terminal ureter
After some hours the calculi was spontaneous elimination.
She was referred to urology service and treated with placement double-J ureteric stent. Postoperatively with good development, she has been asymptomatic since then. After 30 days, was removed the double J catheter and ureteroscopy performed, which showed no abnormalities.
DISCUSSION
Renal pelvis rupture has the same symptoms as renal colic. The most common symptoms are renoureteral colic, flank pain, nausea, and vomiting [1,4]. In physical examination, symptoms similar to abdominal pain pathogenesis, such as pyelonephritis, appendicitis, duodenal ulcer, biliary colic, and cholecystitis, may be seen1.
Urine extravasation is the result of a leakage of the urinary collecting system at any level from the calix to the urethra. This is defined asspontaneous if it is not induced by external trauma, iatrogenic manipulation, degenerative kidney diseases, or previous surgery. Calculi represent the most frequent cause of ureteral and pelvis rupture in the nontraumatic group, but there are rare cases related in literature [5].
No explanation of the mechanism and causes of pelvic rupture has been reported in literature. Theoretically, one possible explanation could be congenital or acquired connective tissue disorders associated with increase of the pressure in the collecting system and tension of the pelvis wall2. It’s important to prevent damage to the collecting system [2].
This sort of condition is associated with other urologic diseases. The most common cause is hydronephrosis, especially when the renal pelvis is fixed because of fibrosis [4].
Ultrasound and intravenous pyelogram has been utilized in diagnosis and differential diagnosis. Intravenous contrast tomography is the most useful diagnostic tool [1-4].
Treatment should be individualized in each case according to underlying pathology. Double J catheter or percutaneous nephrostomy is urinary diversion method to be used especially in the presence of small ruptures [1,2,4]. Open surgery can be an option in difficult cases associated with extensive rupture of renal pelvis [1,2,4].









































































































































{kind=link}