Increased Serum Von Willebrand Levels in Chronic Lymphocytic Leukemia (CLL) Patients Are Related To a Shorter Time to Treatment
- 1. Hematology section of First Department of Propaedeutic Internal Medicine, Laikon General Hospital, National and Kapodistrian University of Athens, Medical School, Athens, Greece
- 2. Laboratory of Hematology & Blood Bank Unit, Medical School, National and Kapodistrian University of Athens, Athens, Greece
Abstract
Chronic lymphocytic leukemia (CLL) is the most frequent leukemia of elderly patients and the role of angiogenesis in CLL pathogenesis and prognosis remains unclear. Angiogenesis may be evaluated by indirect methods such as evaluating von Willebrand factor (vWF) stainig by immunohistochemistry. Here we investigated whether serum vWF levels in CLL patients at diagnosis are related to disease characteristics or prognosis.
Seventy-two (72) CLL patients were studied of whom 52%, 32% and 16% were Binet staged A, B and C respectively. Serum vWF was measured by ELISA (R&D Quantiquine, duo Set) in frozen sera drawn at patients’ diagnosis and in 10 healthy individuals (HI). Forty-three percent never required treatment while 55% required treatment either at the time of diagnosis or during their follow-up. None of the patients presented hemorrhage or thrombosis. Statistical analysis was performed by conventional methods, using the SPSS v.22 software. behavior.
Serum vWF levels ranged from undetectable (0) to 17998 pg/ml (median 4273,8) in patients and from 374,6 to 4422,5 pg/ml (median 2692,7) in HI, the difference being statistically significant (p< 0,05). Patients with serum vWF levels above patients median had a significantly shorter Time to First treatment than the others (p=0,000054). Otherwise, serum vWF levels correlated only with hypogammaglobulinemia (p=0,04).
Our results suggest for the first time, to our knowledge, that serum vWF levels are increased in CLL patients and importantly, that higher vWF levels correlated with a shorter TFT, suggesting that increased vWF levels reflect active neoangiogenesis that in turn, contributes to a more aggressive disease
Keywords
• CLL
• Prognosis
• Serum vWF
CITATION
Tryfou TM, Papaioannou P, Gkioka AI, Alexandropoulos A, Papadatou M (2023) Increased Serum Von Willebrand Levels in Chronic Lympho cytic Leukemia (CLL) Patients Are Related To a Shorter Time to Treatment. J Hematol Transfus 10(2): 1115.
INTRODUCTION
Chronic lymphocytic leukemia (CLL) is the most frequent leukemia of elderly patients. It is usually an indolent neoplastic lymphoproliferative disorder characterized by increased number of small B-lymphocytes expressing CD23 and aberrantly CD5 in the blood. Likely, lymphocytosis is, by definition, present while lymphadenopathy, organomegaly, anemia, thrombocytopenia, susceptibility to infections are typical findings that do not always develop. About 2/3 of patients require only follow-up while the rest 1/3 of patients are symptomatic, have a worse outcome and need to be immediately treated. During CLL course a portion of asymptomatic patients will acquire symptomatic disease needing treatment.
It is well known that neoangiogenesis contributes to disease proliferation and aggressiveness in solid tumors and other hematological malignancies although its role in CLL pathogenesis and prognosis remains unclear. The concept of neoangiogenesis triggering CLL cells proliferation is quite provocative because a large amount of disease mass is freely circulating in blood, albeit in vessels.
Angiogenesis may be evaluated by indirect methods such as measurements of cytokines and other soluble factors that promote vessels formation such as VEGF, BFGF and others; it can also be assessed by direct methods such as microvessels immunostaining of involved biopsied tissues or organs, using frequently CD34 or von Willebrand factor (vWF) [1,2].
The vWF is mainly secreted by endothelial vessels, plays an important role in hemostasis but also contributes to angiogenesis [1].
In the present study, we investigated whether serum vWF levels in CLL patients at diagnosis are related to disease characteristics or prognosis.
PATIENTS AND METHODS
Serum vWF was measured by ELISA (R&D Quantiquine, duo Set) in frozen sera drawn at patients’ diagnosis and in 10 healthy individuals (HI). Measurements were performed according to the manufacturer's instructions. Medical files were reviewed and testing was done after obtaining patients informed consent. Statistical analysis was done by conventional methods, survival curves were drawn by the Kaplan-Meyer method using the SPSS v.22 software and then compared by the log-rank test. P values below 0,05 were considered statistically significant.
Seventy-two (72) CLL patients were studied of whom 33%, 30%, 18%, 7%, 11% and 1% were Rai staged 0, 1, 2, 3, 4 and 5 respectively. Forty-three percent never required treatment while 55% required treatment either at the time of diagnosis or during their follow-up. The median time to first treatment (TFT) was 31 months (range 0-280) while the median follow-up time was 71 months (range 1-230). None of the patients presented hemorrhage or thrombosis.
RESULTS
Serum vWF levels ranged from undetectable (0) to 17998 pg/ml (median 4273,8) in patients and from 374,6 to 4422,5 pg/ml (median 2692,7) in HI, the difference being statistically significant (p< 0,05). Patients with serum vWF levels above patients median had a significantly shorter 6-years TFT than the others (p=0,000054) as shown in Figure 1.
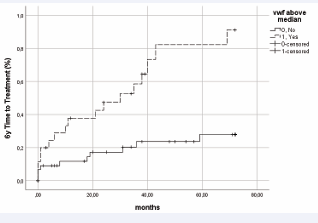
Figure 1: Six-years’ time to first treatment according to serum vWF levels
No correlations were found between clinical characteristics (lymphadenopathy, organomegaly), laboratory findings (white blood cells counts, lymphocytosis, hemoglobin, platelets counts or biochemical routine tests) or Rai staging and vWF serum levels. Serum vWF levels correlated only with hypogammaglobulinemia (p=0, 04).
DISCUSSION
Our results suggest for the first time, to our knowledge, that serum vWF levels are increased in CLL patients and importantly, that higher vWF levels correlated with a shorter TFT, suggesting that increased vWF levels reflect active neoangiogenesis that in turn, contributes to a more aggressive disease behavior. We did not found any correlations between vWF levels and disease variables, except the presence of hypogammaglobulinemia. Hypogammaglobulinemia is frequently encountered in patients with B-cell lymphoproliferative disorders, including CLL. It occurs in about one quarter of newly diagnosed patients but become increasingly seen over the course of the disease and contributes to patients’ sensitivity to infectious agents.
There are very few reports on angiogenesis in CLL [3,4]. It was shown that CLL plasma promotes vWF secretion, and expression in human umbilical vein endothelial cell cultures (HUVECs) [3] and microvessel density was found increased in CLL patients’ bone marrow.
Based on the potential contribution of neoangiogenesis in CLL pathogenesis, anti-angiogenic agents for CLL patients’ treatment seemed promising [5]. Many agents were used but the most interesting were anti-VEGF (Bevacizumab) and IMiDs (lenalidomide); however, as monotherapy, treatment was not as efficient as expected and accompanied with side effects such as cardiovascular complications for the first and flair for the second. Their combination with other agents showed better results. Improved progression free survival was observed with the addition of bevacizumab to chemoimmunotherapy [6]. The same was true with the addition of rituximab to lenalidomide [7,8].
With regard to the effects of vWF serum levels, we did not found any other report than ours in published medical literature. However, an adverse prognostic impact of high serum vWF levels was reported in other B-cell lymphoproliferative disorders such as AL amyloidosis [5] and Waldenstrom’s macroglobulinemia.
We believe that further research on the biologic contribution of angiogenesis and vWF in CLL, as well as their implications in prognosis and hemostasis, are needed for a better understanding and management of CLL patients.







































































































































{kind=link}