Transfusion Induced Hemoglobinopathy: An Underdiagnosed Entity
- 1. Department of Pathology, Pandit B.D. Sharma PGIMS Rohtak, Haryana, India
- 2. Department of Pathology, Pt. BDS, PGIMS, University of Health Sciences, Rohtak
Abstract
HPLC (High performance Liquid Chromatography) is a method of identification and quantification of hemoglobin variant. Transfusion acquired or apparent hemoglobinopathy is now not uncommon entity with the availability of HPLC. Asymptomatic carrier of abnormal hemoglobin variant may donate blood and when such blood unit transfused to another person, it results in erroneous peaks on chromatograms. These peaks are transient in nature and having low percentage of abnormal hemoglobin variant, create a diagnostic dilemma and chances of misdiagnosis. Here, we report a case of such transfusion induced hemoglobinopathy with peak at HbD window. On further workup, history of prior blood transfusion, negative family screening and decrease peak at HbD window on repeat testing after two weeks confirmed the diagnosis.
Citation
Pawar R, Gupta M, Chhabra S, Kataria SP, Singh S (2021) Transfusion Induced Hemoglobinopathy: An Underdiagnosed Entity. J Hematol Transfus 8(2): 1095.
Keywords
• High performance liquid chromatography
• Hemoglobinopathy
• Transfusion
INTRODUCTION
Prevalence of hemoglobinopathies in India is quite high ranges from 3.5% to 15% in different ethnic groups [1]. The estimated average prevalence of thalassemia carrier is 3 to 4% which translates to 35 to 45 million carrier of 1.21 billion populations [2]. Phenotypically silent or asymptomatic carriers lead a perfectly normal life. Being unaware of their abnormal haemoglobin (Hb) variant these asymptomatic carriers might donate blood. In India, on routine blood screening process no special test is applied to screen the donated blood unit for hemoglobinopathies. When such blood units are transfused to recipient it might result in erroneous peaks on High Performance Liquid Chromatography (HPLC) (BioRad Variant II, β-thalassemia Short Programme chromatograms, that is known as apparent hemoglobinopathies or transfusion induced hemoglobinopathy.
CASE PRESENTATION
A young woman aged 18 years, present to gynaecology OPD with chief complaints of menorrhagia, weakness and fatigue from the past 15-20 days. Laboratory investigations including complete blood counts (CBC) and peripheral blood film examination were done. Hemogram showed Hb 3.6 gm% with microcytic hypochromic picture and marked anisopoikilocytosis, Hb HPLC of the patient showed raised HbF level of 10.3% with HbA0 58.5%, HbA2 1.4% and a peak in D - window of 20.5% with at retention time of 4.07 min. The expected percentage of HbD in heterozygotes is ~40% but in our case it was significantly low. Family study was performed. Both the parents and one sibling were found normal on HPLC. In view of low percentage of abnormal HbD variant and negative family screening lead us to enquire about history of recent blood transfusion. It was found that she received multiple blood transfusions from different places in view of her severe anaemia. Also, we found that the sample processed for HPLC was drawn after two days of transfusion.
Due to low percentage of HbD, normal family screening and history of recent blood transfusion raised suspicion of transfusion induced hemoglobinopathy. On follow up, repeat HPLC was performed (after two weeks), which revealed decrease in percentage of HbD from 20.5% to 8.2% and HbF from 10.3% to 5.6%. This fall in the peak on HPLC chromatogram nearly solved all the mystery and confirmed our diagnosis of apparent transfusion induced hemoglobinopathy.
Since patient received multiple transfusions from different places it was not feasible to trace the exact blood unit from which the abnormal haemoglobin was transfused.
DISCUSSION
Apparent hemoglobinopathy or transfusion associated abnormal peak on HPLC chromatogram are not uncommon in a country like India, where such a high prevalence of carrier state exists. On this entity largest case series was conducted by Kozarski et al [3] with 52 incidences of transfusion induced hemoglobinopathy associated with peak in 32 recipients. The donor are mostly carrier or heterozygous state of HbS, HbD, HbE who remain clinically silent. These carrier has near normal level of haemoglobin which made them acceptable donor on blood donor screening test. Special test to screen the abnormal haemoglobin variant are mainly HPLC and molecular testing. In developing country like ours with limited resources, it is not possible to screen all donor units for abnormal hemoglobin. When such blood units are transfused it result in abnormal peak on chromatogram. Fortunately, such transfused units rarely causes serious life threatening complications to the recipient, only one case report by Nowak et al[4] in the literature. In their study, a neonate developed multiple renal and splenic infarcts after transfused with blood from a sickle cell trait donor [Figure1,2].
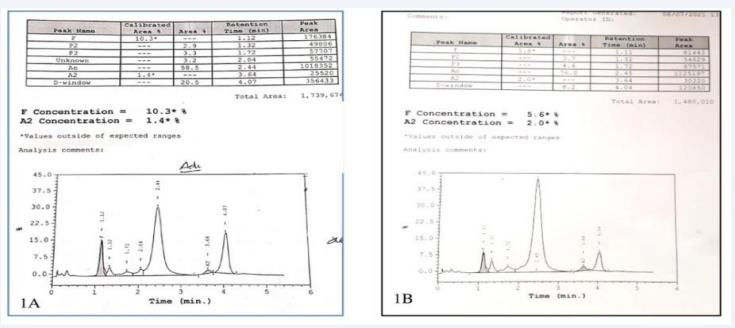
Figure 1 Hemoglobin high-performance liquid chromatography of patient (1A) showing a peak in D-window of 20.5% with a retention time of 4.07 min (1B) After 2 weeks the peak in D-window reduced to 8.2%.
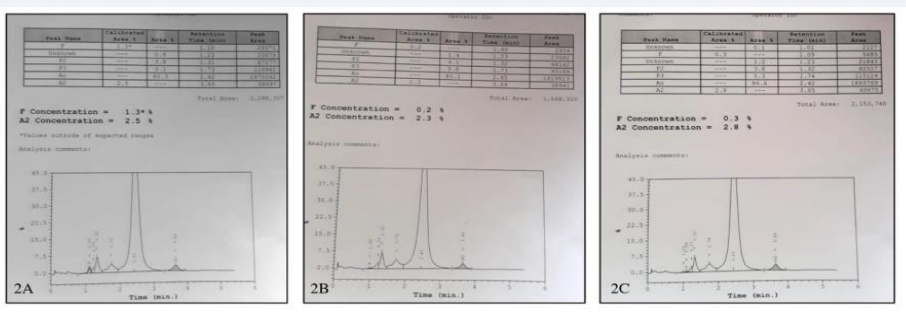
Figure 2 Hemoglobin high-performance liquid chromatography of (2A) Father (2B) Mother and (2C) Brother showing normal chromatogram.
Being a part of preanalytical error, it create a lot of diagnostic dilemma to even most experienced personnel. The main reason for the diagnostic dilemma is the low percentage of abnormal haemoglobin variant which does not fit even for the heterozygous states mostly. As in our case the percentage of abnormal haemoglobin variant was low i.e. 20.5% with retention time of 4.07 minutes. Similar study by Jain et al [5] reported low percentage of Hb D i.e. 10.2% with retention time of 4.06 minutes, Somasundaram et al[6] also reported peak in D-window of 8.9% with RT of 4.07 minutes. These transfused abnormal Hb variant are transient in nature and their percentage decreases with time and eventually completely disappear from the blood, as the lifespan of transfused red cells is over.
When such incidental small peaks are detected on chromatogram they should be correlated with retention time, their shape, with other corresponding peaks like unstable alpha chain, delta chain variant, any technical artefact. Kozarksi et al [3] highlight the significance of technical artefact in chromatogram that adds to diagnostic confusion. In his largest study ever, he found one case with appearance of HbC from the previous run sample eluted as a small peak (6.5%) in the succeeding chromatograms. So, one should be aware of all these possible technical artefacts that contribute to erroneous results on chromatogram.
A detailed history regarding blood transfusion prove very helpful in solving such mysterious cases. HbD values in our patient may be related to reduced gap between transfusion and HPLC testing. Pore et al [7] recommend HPLC testing should be done prior to transfusion or 3 months post transfusion period to avoid such diagnostic confusion on chromatogram.
Testing the donor unit may be done to confirm the presence of abnormal Hb variant in the donor. Nowak et al [4] and Lippi et al [8] also recommended screening of blood donor unit for hemoglobinopathy. But sometimes this retrospective tracing of donor blood unit might not be very feasible if the patient receive multiple transfusions from different places or if donor segment discarded from blood bank.
Hemoglobinopathies being genetic diseases, so family screening carries a great significance on reaching to a conclusion. Both parents and a sibling came out absolutely normal in our case and aids in solving the puzzling nature of low percentage of HbD.
To conclude, for persons who are dealing with practice of reporting HPLC findings, following things are helpful in reaching out to diagnosis – Family study, low percentage of Hb variant, decline or disappearance of peak and history of prior transfusion. Misdiagnosis of this entity could lead to unnecessary testing, treatment and counselling. To avoid this confusing entity, HPLC sample should be tested either prior to any blood transfusion or three months post transfusion period. Being a genetically transmitted disease, we also recommend to notifying the donor about abnormal Hb variant, wherever retrospective tracing is possible at blood donor centres, so that donor could be benefitted for proper future counselling and family planning.







































































































































{kind=link}