An Indolent Presentation of a High Risk Colloid Cyst
- 1. Department of Neurosurgery, The Institute of Neurological Sciences, UK
Abstract
We present a 62 year old female patient who gradually lost cognitive function, followed by gait disturbance and then urinary incontinence over the course of one year. She was investigated for potential Parkinson’s disease given the absence of headache or visual disturbance. MRI imaging revealed a large 2cm colloid cyst within the anterior part of the third ventricle causing hydrocephalus. This indolent presentation, for what radiologically is classified as high risk colloid cyst, runs contrary to classical presentation for this tumour.
CITATION
Kumar A, Hassan S (2023) An Indolent Presentation of a High Risk Colloid Cyst. J Neurol Disord Stroke 10(3): 1208.
ABBREVIATIONS
MRI: Magnetic Resonance Imaging; FLAIR: Fluid Attenuated Inversion Recovery
CASE PRESENTATION
Colloid cysts are a benign intracranial tumour, often located within the third ventricle. Although they represent only 2% of intracranial tumours, they account for 20% of all intraventricular neoplasms [1,2]. Colloid cysts are believed to be a developmental malformation and as such the majority of them are discovered incidentally [3]. A 62 year old previously fit and well woman initially noted symptoms of forgetfulness a year prior to presentation. This then went on to affect her ability to work. Thereafter, she gradually developed problems with gait initiation and started to have falls. Latterly she developed urinary incontinence. She denied any headache or visual disturbance. On examination the patient required a wheelchair to mobilise indoors. She was able to stand but had the classical “magnet gait” of normal pressure hydrocephalus due to problems with gait initiation. There was no papilledema but an upward gaze palsy was present. Sensory and motor function in the limbs were normal without upper motor neurone signs. Magnetic resonance imaging revealed a large 21mm colloid cyst of the anterior portion of the third ventricle with associated hydrocephalus. According to the validated Colloid Cyst Risk Score this was a “high risk” symptomatic lesion due to the patient’s age, size of lesion, MRI FLAIR hyper-intensity and location, carrying a risk of death of 3.1% [4]. The patient underwent endoscopic resection of the cyst with pathology results confirmed a colloid cyst of the third ventricle with evidence of organised internal haemorrhage (Figures 1-5).
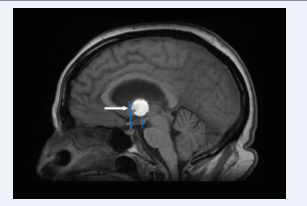
Figure 1: Saggital T1-weighted magnetic resonance imaging (T1W-MRI) showing large colloid cyst (arrow) occupying Risk Zone I- from the lamina terminalis (solid blue line) to a vertical line drawn from the mammillary body and tangential to the massa intermedia (dotted blue line)
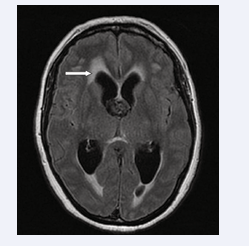
Figure 2: Axial Fluid-attenuated inversion recovery (FLAIR) MRI showing hydrocephalus with trans-ependymal oedema (arrow)
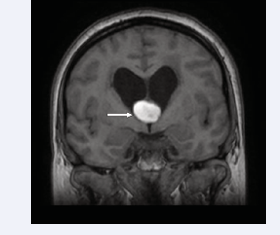
Figure 3: Sagittal T1W-MRI showing colloid cyst obstructing both foramen of Monro (arrow).
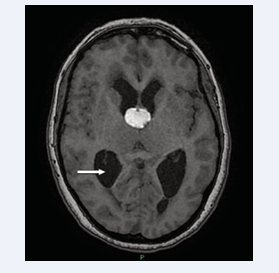
Figure 4: Axial T1W-MRI showing colloid cyst causing obstructive hydrocephalus (arrow).
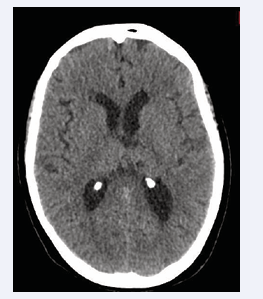
Figure 5: Post-operative Axial CT head showing resection of the colloid cyst and resolution of hydrocephalus
The patient’s mobility, continence and cognitive function improved over a period of months. Our patient is a reminder to the clinician that large, high-risk colloid cysts of the third ventricle can present without headache and in a chronic fashion.







































































































































{kind=link}