Assisted Cycle Therapy Improved Executive and Motor Functioning in Young Adult Females with Attention-Deficit Hyperactivity Disorder: A Pilot Study
- 1. College of Health Solutions, Arizona State University, USA
- 2. Department of Kinesiology, Mississippi State University, USA
Abstract
Research is limited on the link between exercise and motor function in the attention deficit hyperactivity disorder (ADHD), population and has not been examined following Assisted Cycle Therapy (ACT). Five adult females with ADHD (age = 21.4 + 2.3), were randomized into either 30 minute Voluntary cycling (VC), or Assisted Cycling Therapy (ACT). Cycling exercise was performed 3x/week for six weeks. Voluntary cycling consisted of cycling sessions at a voluntary rate and the ACT consisted of cycling sessions at an assisted rate from a motor 35% greater than their voluntary rate. Within the ACT group improvements were demonstrated pre and post 6 weeks in activation, planning, effort, attention, memory, and bimanual dexterity. These results are discussed with respect to neurotrophic factors in the prefrontal cortex. Assisted Cycle Therapy is effective for improving executive and motor functioning in young adult females with ADHD, which will improve the quality of their life.
Citation
Ringenbach SDR, Birchfield N, Nam K, Chen CC (2022) Assisted Cycle Therapy Improved Executive and Motor Functioning in Young Adult Females with Attention-Deficit Hyperactivity Disorder: A Pilot Study. J Neurol Disord Stroke 9(1): 1191.
INTRODUCTION
Disorganization, recklessness, distractibility, restlessness, and dysregulated emotions are among some of the traits that disrupt the lives of many individuals with attention deficit hyperactivity disorder. Attention deficit hyperactivity disorder (ADHD), is recognized worldwide as one of the most prevalent developmental disorders [1]. While commonly considered a childhood disorder, according to the National Institutes for Mental Health, ADHD affects approximately four percent of adults in the United States alone, with an estimated 41 percent being classified as severe. Kessler et al. [2] has reported among adult females aged 18-44, three percent are affected by the disorder.
Although it was previously thought that most cases of ADHD resolved before adulthood, it is now estimated that 50-60% of children diagnosed with ADHD in childhood continue to suffer from the disorder into adulthood [3]. ADHD is highly associated with behavioral dysfunction in children, but in adults the disorder commonly disrupts cognitive, emotional, and social functioning. Adults with ADHD are more likely to experience joblessness due to excessive errors, lateness and absenteeism, interpersonal and relationship difficulties, and are at a significantly higher risk for engaging in risky behaviors and substance abuse [4].
The estimated annual costs associated with ADHD are approximately $42.5 billion, including health care, education, disciplinary costs, loss of work, and justice costs [5]. This is a tremendous financial burden that is not only assumed by those directly affected by ADHD adolescents but also by government agencies. Health care expenses for diagnosed individuals, including medications prescribed to treat the illness, exceed $13 billion annually [6]. Medications, such as Ritalin (i.e., methylphenidate), and Adderall (i.e., amphetamine), Class II stimulant narcotics, are commonly prescribed to treat the symptoms associated with ADHD, costing $1.3 billion per year. These medications target the dopaminergic pathways in the brain, in order to minimize the dysfunction caused by ADHD, by acting on the pathway to increase the production and availability of dopamine in the prefrontal region of the brain [7,8]. Dopamine is an essential neurotransmitter that plays a role in executive and motor functioning in the brain and has been found to be significantly less available in the ADHD brain [9].
Executive functioning is a collective term used to describe “high-level cognitive processes that control and regulate other lower-level processes” [10]. Brown [11] has created a conceptual model of executive function which includes six primary clusters of cognitive processes; Figure 1. (1) Activation- describes the executive functions of organization, prioritization, and activation; (2) the Focus cluster is primarily involved in focus, sustained attention, and the ability to shift attention; (3) Effort is related to alertness, sustaining effort and processing speed; (4) the Emotion cluster helps with managing frustration and modulating emotions; (5) Memory deals with utilizing working memory and accessing recall; (6) and the Action cluster is involved with monitoring and self-regulation. Brown [11,12] has suggested individuals with ADHD have impaired executive function as a result of impairments in the cognitive clusters. For example, when individuals experience weakness in the activation cluster, issues with procrastination, task initiation and organization are areas that interfere with cognitive performance [13]. Often times individuals understand what they need to do they just have difficulty with the initiation process. When weaknesses are observed in the focus cluster, stick-to-itiveness is often times a major deficiency [13]. Even when individuals recognize the importance of focusing on a task for an appropriate amount of time needed to complete the task, executing this seems impossible. Distractibility is often times heightened and it is common to become hyper-focused on background noises, thoughts or even the environment [13]. Thus, executive function is imperative for inhibition, attending, and emotion regulation, as well as organization, planning and execution [11]. ADHD creates deficits in neuropsychological functioning, most commonly identified as executive dysfunction [14,15]. Executive dysfunction often leads to dysregulated processes and may be due to a reduction in the production and availability of dopamine in the brain [16].
In addition to impaired executive functioning, the ADHD population experiences the effects of dysfunctional motor control [17]. Motor dysfunction, observed in manual dexterity tasks and handwriting skills, is reported to be present in 50 percent of individuals with ADHD [18,19]. Impaired motor control has also been known to affect gross motor movements typically observed as clumsiness, in ADHD populations [20]. Clumsy behaviors associated with ADHD are often attributed to inattention and distractibility but may be better understood as impairments in motor control and movement coordination [20]. Motor coordination dysfunction is not currently recognized as a component of the ADHD diagnosis based on DSM-V criteria. However, in many other countries, ADHD is referred to as Hyperkinetic Disorder and includes the impairment of motor development in addition to the inattention, impulsivity and hyperactivity components when diagnosing the disorder [20].
Executive and motor functioning develops throughout childhood as the brain develops and this process may follow an abnormal trajectory in children and adolescents with ADHD [15,20]. Castellanos [21] has suggested that the brain of an individual with ADHD has developmental lag of approximately two years. However, more recent studies suggest, that the brain is actually smaller in those with ADHD, with a total brain volume reduction of approximately 3-5% [15]. Although a reduction in brain size may not adequately explain the differences between an ADHD brain and an unaffected brain, it is the regions of the brain that are smaller that deserve closer attention.
Subcorticol regions of the brain, which include the nucleus accumbens, caudate nucleus, the midbrain, and the prefrontal cortex are the regions that are most impacted by dopamine [9]. Molecular imaging studies have shown that within the ADHD brain, these areas not only produce lower levels of dopamine, they actually house fewer dopamine receptors [9]. The receptors are important for accepting neurotransmitters released in the brain cells. Without the presence of the receptors, the chemicals have no distinct pathway to follow. Lower production of dopamine and less neural availability of the neurotransmitter may be one explanation for many of the symptoms associated with ADHD. Distractibility, attention sustainability, emotional regulation and behavioral regulation are all highly influenced by the dopaminergic pathways [22]. Although ADHD medications target these areas of the brain and increase dopamine production, alternative methods of treatment should be considered for those who wish to avoid the potential for complications associated with amphetamine (e.g., Adderall and Vyvanse), and methylphenidate (e.g., Ritalin), use. Understanding the role of the structures in the brain is important when considering how to treat the symptoms associated with ADHD. Exercise may be one potential alternative treatment that could improve executive and motor functioning by increasing dopamine production as well as proteins specific to neurogenesis in ADHD individuals in a natural way.
TREATMENT RECOMMENDATIONS
The use of psychostimulant medications is the most common treatment for controlling the symptoms of hyperactivity, impulsivity and inattention in individuals diagnosed with ADHD. The Center for Disease Control reports that 50% of diagnosed ADHD children and adolescents are being treated with prescription medication [23]. Methyphenidate (Ritalin), and l-amphetamine (Adderall), the two most commonly prescribed ADHD medications, act on the subcorticol regions of the brain to increase dopamine production and concentration of the neurotransmitter in these regions [24]. Psychostimulant medications have also been found to modulate the expression of BDNF, elevating BDNF activity in the brain [25,26]. In addition, BDNF has been found to modulate neuroadaptations and locomotor activity through the dopaminergic pathways [25]. While stimulant use has proven to be efficacious, long-term stimulant use is not without consequences. Some researchers have observed the effects of these drugs through animal observation. Tang [24] have looked at the negative impacts of long-term stimulant use in rats and have found that tolerance, withdrawal and behavioral sensitization actually reduce natural dopamine production, facilitate the need for greater amounts of the drug, and can lead to chemical dependence. Although there have been a few studies looking at whether or not stimulant use causes structural changes within the adolescent brain, there is no information on long-term use and dependency, or, disruption of the developmental process.
EXERCISE AND EXECUTIVE AND MOTOR FUNCTIONING
Sedentary behavior is often associated with a plethora of negative health consequences including cognitive decline. This may be particularly concerning in sedentary populations with a genetic predisposition for cognitive impairments, such as individuals with ADHD. In recent years, the connection between brain health and exercise has been highlighted as an important determinant of health. Research indicates there is a positive relationship between adhering to a regular physical activity regimen and improved cognitive function [27]. Verret [28] have found that physical activity has a positive impact on motor performance, behavioral scores which evaluated social skills, attention, thought processes, and information processing.
Some researchers have specifically looked at the benefits of exercise as a means of improving functioning within individuals with ADHD. Verret [28] have shown that significant behavioral and cognitive function improvements were seen after a physical activity program was implemented for a period of 10 weeks. Improvements were observed in informational processing, motor performance, behavioral adaptability, and attention within the ADHD population. Interestingly, there were no significant differences in the improvements in fitness parameters between groups; the only improvement was found in processes involving executive functioning. Dishman [29] have looked at the effects of exercise on both emotional and cognitive processes and have found that exercise is more positively associated with processes that require higher-level executive control, such as scheduling, planning, and task coordination; changes in the brain’s plasticity, down to the intercellular level, were also observed, and are thought to be responsible for improvements in learning and memory.
Exercise has been shown to influence cognition, executive functioning and the dopaminergic pathways in ADHD individuals, positively influencing their ability to plan, execute and perform executive functioning tasks [30]. Treadmill exercise has been found to increase dopamine levels and dopaminergic transmission in regions of the brain affecting cognition and motor function [31]. Brain derived neurotrophic factor, BDNF, is a protein responsible for neurogenesis, the growth of neurons in the brain. Chemicalof post-synaptic neurons. Physical exercise has been shown to increase levels of BDNF by approximately 32 percent [32].
Assisted Cycle Therapy is a mode of aerobic exercise that is enhanced by the use of motorized equipment. The mechanical assistance enables a participant to achieve and maintain an exercise speed that is greater than a preferred self-selected, voluntary speed [33]. ACT has been evaluated in persons with Parkinson’s disease, a progressive neurogenerative disorder resulting in the degeneration of the dopaminergic pathways, and found to enhance motor function above and beyond that of voluntary exercise [33]. Ringenbach [34] have demonstrated similar patterns of improvement in persons with Down syndrome, in addition to improvements in cognitive functioning. As can be seen in Figure 1,
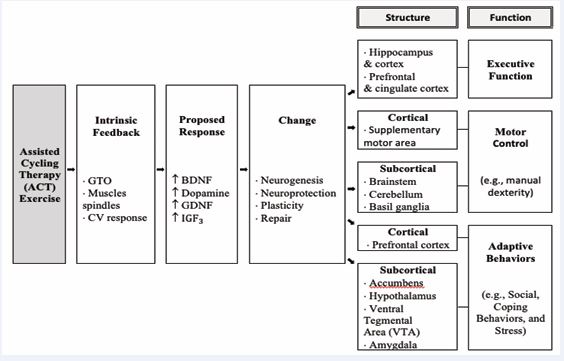
Figure 1 Model of structure and mechanisms responsible for ACT.
changes at the molecular level, i.e., altered dopaminergic pathways, are thought to be affecting the function of the prefrontal and motor cortices through increases in afferent neurological signaling [33,34]. Due to these findings, Assisted Cycle Therapy is an innovative approach to improving neuropsychological function in the ADHD brain. Assisted Cycle Therapy could be a non-pharmaceutical approach to treating ADHD. Drug use often carries an excess of negative side effects that would not accompany exercise. Based on previous research in other populations with prefrontal cortex deficits (e.g. Down syndrome), and dopamine deficits (e.g. Parkinson’s disease), the primary hypothesis of this states that Assisted Cycle Therapy will elicit significantly greater improvements in measures of executive function compared to Voluntary Cycling in adult females diagnosed with ADHD. The secondary hypothesis states Assisted Cycle Therapy will elicit significantly greater improvements in measures of functional motor behaviors compared to Voluntary Cycling in adult females diagnosed with ADHD.
METHODS
Participants and Study Design
Eight female volunteers between the ages of 18 and 24 were screened for attention deficit hyperactivity disorder. Selection was limited to individuals with a diagnosis of ADHD by a qualified health care professional; met Physical Activity Readiness Questionnaire (PAR-Q), criteria in order identify if the participant was positive for risk factors associated with aerobic exercise; had no physical limitations for cycling; had no history of trauma or injury to the brain; did not meet current physical activity guidelines. Participants were recruited through fliers posted at the Arizona State University Downtown and Tempe campuses as well as word of mouth. The Arizona State University Institutional Review Board evaluated and approved all procedures. Each participant provided informed consent prior to participation in the study.
Participants were randomly assigned to either the ACT or Voluntary Cycling group. A one group pre-test/post-test design with two treatment groups was administered over a period of six weeks to inactive, female participants with ADHD. An evaluation and pre-test was conducted on both groups to obtain demographic and baseline executive and motor function assessment data. A final evaluation and post-test session was conducted at the end of six weeks to assess any changes in executive and motor function.
Voluntary Cycling (VC): This group consisted of participants cycling on a stationary cycle ergometer at a voluntary speed for a duration of 30 minutes. The rate of cycling (cadence, rpm’s), was voluntarily selected by the participant. Each cycling session was preceded by a five minute warm-up followed by a five minute cool down. Heart rate and cadence were monitored for the duration of the session.
Assisted Cycle Therapy (ACT): This group consisted of participants cycling on a stationary cycle ergometer at an assisted predetermined speed for a duration of 30 minutes. In order to determine the cadence at which each participant was to cycle, the participant cycled at a voluntary speed for five minutes during which an average voluntary cadence was observed and recorded. The average cadence was then increased by 35% to determine the assisted rate at which the motor was to be set. Each cycling session was preceded by a five minute warm-up followed by a five minute cool down. Heart rate and cadence were monitored for the duration of the session,
Exercise Equipment and Evaluation
Cycling Equipment: The Theracycle Model 200 motorized cycle, developed for use in populations with limited mobility, was used in this study in conjunction with the Power Control Monitor (PCM). The PCM stores HR, power produced by the participant, power contribution of the motor, and cadence. There were also measures in place to ensure participant safety such as an emergency stop tether and an excessive load detector within the motor. The motorized component of the Theracycle was only used in the ACT group. Cadence (revolutions per minute), was manually recorded every minute during the 30 minute exercise session.
Heart rate: The participants wore a Polar HR monitor (Mode S 610i; Polar Electro, Finland), in order to measure heart rate during exercise. This model transmitted data via a short-range radio to the PCM in order to collect data during the 30 minute exercise session. Average heart rate data was manually recorded every minute of the exercise bout.
Exercise Intensity: Predicted heart rate values were calculated to determine the appropriate intensity of the exercise administered to the participants. Target heart rates were calculated based on a percentage of maximal heart rate. Maximal heart rate was calculated using the following formula: Max HR = 207 – (0.7 X age). The target heart rate was calculated using the following formula Target HR = (HRmax – HRrest ) X % desired intensity (60-80%) + HR Rest. Participants were encouraged to maintain an exercise intensity to keep their target heart rate close the calculated value.
Executive and Motor Function Measures
Each participant was evaluated for deficiencies in executive function based on Brown’s model of executive function. Each cluster of cognitive function was assessed pre and post intervention with the following tasks; (1) Activation and planning- Tower of London; (2) Focus, attention, and set shifting- Stroop Test; (3) Sustaining effort and processing speed- Verbal Fluency task; (4) Emotion regulation- Difficulty with Emotion Regulation Scale; (5) Working memory- Auditory Number Memory task; (6) Action- Self Regulation Questionnaire.Tower of London: Cognitive planning represents the higher order processes necessary for problem solving and adaptation involving interaction between the prefrontal lobe, cortical and sub-cortical regions of the brain [35]. The Tower of London (r = .81), assesses cognitive planning and problem solving skills through a series of tasks. The researcher placed three colored balls onto three pegs always in the same starting position; the participant was shown a picture of which the colored balls were to be positioned (i.e. goal pattern), and was given a total number of moves in which they were to replicate the goal pattern. The time for completion, attempts, and the number of moves the participant made were recorded. Stoop Test: Focus, attention, and set-shifting (i.e., the ability to shift cognitive processes when responding to environmental change), are characteristics of the cognitive process of activation. Cognitive activation involves being exposed to a stimulus and determining an appropriate response, requiring a degree of interference control requiring focus, attention and set-shifting [36,37]. The Stroop test (r = .87), has been widely used to assess and quantify response inhibition and interference control deficiencies within the ADHD population. The participant was given a set of cards and instructed to read a set of baseline words displayed in black ink, name a set of colored blocks, and read a set of incongruent color words as quickly as they could in 45 seconds. The number of responses (maximum of 100), as well as the time of completion was recorded for each task.Verbal Fluency: Cognitive processing requires effort, planning and self-monitoring as a means of sustaining cognitive behavior involving the frontal lobe regions of the brain [38]. The Verbal Fluency task (r = .92), assesses cognitive output and the process of response inhibition. The objective for the participant was to produce as many words belonging to a given category, semantic or phonemic, within 60 second time periods which were recorded by the researcher.
Difficulties with Emotion Regulation Scale: The domains of emotion regulation involve affect regulation and behavioral control. Individuals with ADHD have a greater propensity for aggression and dysregulated emotional responses, characterized as high intensity behaviors as well as high levels of both positive and negative behaviors [39]. The Difficulties with Emotion Regulation Scale (r = .88) assess the degree to which individuals are able to regulate their emotional behaviors [40]. The DERS questionnaire was administered by the researcher and answered by the participant.
Auditory Digit Span: Working memory underlies several cognitive abilities, involving the short-term ability to retain and manipulate information, and has been found to be impaired in individuals with ADHD [41]. The Auditory Digit Span task (r = .80), required the researcher reading aloud a sequence of digits, each of which became increasingly longer, at a rate of one number per second. The task consisted of forward and backwards trials. During the forward trials the participant is asked to repeat the sequence exactly as it was given. During the backward trial the participant was instructed to repeat the sequence in reverse order. Responses were recorded and scored by the researcher.
Self-Regulation Questionnaire: Self-regulation involves the ability to develop, implement and maintain behavior and may be hindered due to one or more deficits in the following processes; receiving relevant information, evaluating the information, triggering change, searching for options, formulating a plan, implementing the plan, and assessing the plan’s effectiveness [42,43]. The self-regulation questionnaire (r = .94), was administered by the researcher and answered by the participant
Purdue Pegboard: Motor and movement coordination processes involving fine and gross motor control will be assessed by evaluation of manual dexterity. The Purdue Pegboard (r = .76), assess fundamental motor limitations through the evaluation of intra- and inter-limb movements and has been used to detect neuropsychological deficits. The tests consisted of three trials and required the participant to unimanually and bimanually assemble pins, washers and collars, as modeled by the researcher. The objective was to assemble as many sets as possible during a timed trial.
Statistical Analysis
Statistical analyses were conducted using SPSS software, version 21 (SPSS 21.0 IBM Corporation, Armonk, New York, USA). Data is presented as mean score values, plus/minus the standard deviation (SD). All data was analyzed for normal a distribution using the Shapiro-Wilk normality test (p > 0.05). All data was normally distributed and no data transformation was necessary. Statistical analyses were conducted for each measure of executive and motor function; Tower of London, Stroop Test,Verbal Fluency, DERS, Auditory Digit Span, SRQ, and Purdue Pegboard. One-sample t-tests were conducted to test for mean differences of pre and post intervention assessments with each treatment condition evaluated separately. A one way ANOVA was used to test for mean differences between conditions. P values were calculated based on the assumption of the two-tailed hypothesis; values less than 0.05 were considered statistically significant.
RESULTS
Quantitative Data
Eight female participants were screened for this study of which six met the ADHD and physical activity criteria. Five of the six participants completed the study. One participant dropped out of the study due to scheduling difficulties. Participant characteristics are presented in Table 1.
|
Table 1: Participant demographic information (mean + SD; N=5). |
|
|
Sex (M/F) Age (Years) Height (inches) Weight (lbs.) Physical Activity (Y/N) Medication Use (Y/N) Handedness (R/L) |
0/5 21.4 (+ 2.3) 65.0 (+ 1.9) 151.8 (+ 50.1) 0/5 5/0 5/0 |
There were two post-intervention between group executive function assessments that were found to be statistically significant. As can be seen in Table 2 and Figure 2, for the Tower of London task the results were significantly higher in the ACT group compared to the VC group based on the number of correct moves (MACT= 51.0 + 3.0, p = 0.013 vs. MVC = 35.7 + 3.1 p = .025) following 6 weeks of ACT.
|
Table 2: Comparison profile of post-intervention executive function and motor function outcome measures between two groups, (N=5); * statistically significant, p < 0.05. |
|||||
|
Profile of Outcome Measures |
|||||
|
|
Measure |
Voluntary Exercise |
Assisted Exercise |
Mean Difference (SD) |
P value |
|
Executive Function |
|
|
|
|
|
|
Activation |
Tower of London - Executive Time |
308 |
198.7 |
109.3 (+75.6) |
.110 |
|
Planning |
Tower of London - Moves |
40.5 |
50.1 |
10.5 (+ 6.2) |
.025* |
|
Focus/Attention |
Stroop Test - Colored Block |
71.5 |
83.7 |
12.2 (+ 11.5) |
.307 |
|
Set Shifting |
Stroop Test - Incongruent Color Word |
43.5 |
53.7 |
10.2 (+ 12.1) |
.437 |
|
Effort |
Verbal Fluency - Semantic |
42.5 |
48.7 |
6.2 (+ 10.3) |
.590 |
|
Processing Speed |
Verbal Fluency - Phonemic |
41.0 |
42.0 |
1.0 (+ 8.9) |
.921 |
|
|
Verbal Fluency - Combined |
83.5 |
90.7 |
7.2 (+ 16.2) |
.695 |
|
Emotion Regulation |
DERS |
98.0 |
72.3 |
25.7 (+ 23.3) |
.281 |
|
Working Memory/ Attention |
Auditory Digit Span - Forward |
10.0 |
13.0 |
3.0 (+ 1.2) |
.065 |
|
Working Memory |
Auditory Digit Span - Backward |
6.5 |
9.7 |
3.2 (+ 1.8) |
.011* |
|
Self Regulation |
SRQ |
206.5 |
270.3 |
63.8 (+ 55.5) |
.254 |
|
Motor Function |
|
|
|
|
|
|
Manual Dexterity |
Purdue Pegboard - Right Hand |
15.8 |
19 |
3.2 (+ 2.5) |
.207 |
|
|
Purdue Pegboard - Left Hand |
14.8 |
17.1 |
2.3 (+ 2.2) |
.324 |
|
|
Purdue Pegboard - Both Hands |
26 |
28.4 |
2.4 (+ 1.7) |
.073 |
|
|
Purdue Pegboard - Right, Left, Both Combined |
56.7 |
64.0 |
7.3 (+ 5.6) |
.151 |
|
|
Purdue Pegboard - Assembly |
8.3 |
11.1 |
.217 |
|
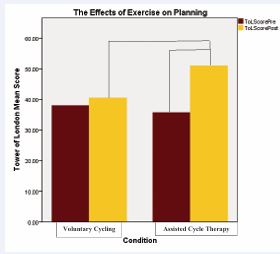
Figure 2 Mean score based on the number of attempts made in order to achieve the goal pattern as a function of Group (i.e., VC, ACT), and Time (i.e., pre, post); statistically significant, p < 0.05.

Figure 3 Working memory assessed using a backward auditory digit span task as a function of Group (i.e., VC, ACT), and Time (i.e., pre, post); statistically significant, p < 0.05.
Mean scores (+ SD) based on number of correctly repeated sequences for the backward auditory digit span task were also significantly higher in the ACT group compared to the VC group, p = 0.011 (6.0 + 1.0 vs. 9.7 + 0.6, p > 0.05, respectively), (Table 2, Figure 2). There were no other statistically significant findings between groups (Table 2).
There were also significant differences between several pre and post executive and motor function assessments within ACT. As seen in Table 3, mean scores (+ SD) for the Tower of London execution time were significantly lower than post 6 weeks of ACT. Tower of London scores based on the number of correct moves and attempts were significantly higher post 6 weeks of ACT (Table 3). Similarly, semantic verbal fluency scores based on the number of recorded responses were significantly greater post 6 weeks of ACT. Both forward and backward auditory digit span scores, based on the number of correctly repeated sequences were significantly higher post 6 weeks of ACT. Mean scores for the bimanual Purdue Pegboard task were also significantly greater post 6 weeks of ACT (Table 3). There were no statistically significant pre/post differences in executive and motor function assessments found within the Voluntary Cycling group (Voluntary group in Figures and Table 2).
Qualitative Data
Medication recall was assessed prior to beginning each cycling session. All five participants reported taking medication on a daily basis prior to the exercise intervention, of which four out of the five, 80%, discontinued medication use within one week of beginning the cycling intervention; of those who reported discontinuance, three, 60%, also reported fewer noticeable occurrences of inattention and distraction.
DISCUSSION
This is the first study, to our knowledge, that has examined cognitive and motor function following a 6 week intervention of either Assisted Cycle Therapy (ACT), or Voluntary Cycling (VC), in adult females with ADHD. This is important to determine if exercise as a non-pharmaceutical intervention could improve cognitive and motor function that would improve their quality of life through improving activities of daily living. Consistent with our hypothesis, one of the main findings of this research indicates that six weeks of ACT three times per week significantly improved functioning in activation, one of the cognitive clusters associated with executive functioning. According to Brown’s model of executive function, the activation cluster consists of the cognitive abilities for planning and activating to work. Activation, organization and planning are considered to be major impairments for individuals with ADHD [44,45].
Cognitive planning
Improvement in the mean score for the Tower of London task was significantly greater in the ACT group compared to the VC group. The observed improvements were insignificant and to a lesser degree in the voluntary exercise group. While there have been no previous studies designed to evaluate the effects of chronic bouts of assisted exercise on these cognitive activation characteristics in ADHD, acute bouts of aerobic exercise have been found to be a significant predictor of better performance as well as facilitate significant change during cognitive planning in typical populations [15,46]. Furthermore, our results are consistent with chronic ACT interventions improving executive function in other populations with prefrontal deficits. The findings of this study are consistent with the research in that there were improvements in reaction time and inhibitory control following 8 weeks of ACT but not Voluntary Cycling in adolescents with DS [47]. For example, improvements in inhibition, cognitive planning and set switching were reported after 20 min acute sessions of ACT but not VC and No Cycling (NC), in adolescents with ASD.
Memory
Another main finding of this study is that it shows significant improvements in the memory cluster for the assisted exercise group when compared to the voluntary group. Brown’s model implicates working memory and recall as the primary cognitive characteristics for this cluster. Working memory is another cognitive impairment frequently observed in individuals with ADHD [48].
There was no significance in mean scores between groups for the forward task (i.e. short term memory), but a significant effect was observed on the backwards task (i.e. working memory). Within each group, improvements were also observed on both the forward and backwards tasks, significant only within the ACT group. This is consistent with previous research that found that working memory is significantly improved after one 30 minute bout of aerobic exercise in typical people during tasks requiring increased working memory capacity [49,50]. While the research appears to be limited to acute bouts of exercise and has not been evaluated specifically in ADHD, the findings of this study are consistent with improvements in working memory found in typical population. Similarly, an 8 week study was conducted comparing ACT and VC in adolescents with DS and measured memory [51]. The results found that only working memory, not short term memory improved in the ACT group and not in a VC or NC group, which supports the suggestion that ACT may increase neurogenesis/neuroplasticity to the prefrontal cortex.
Executive function: Within group effects
While there were no other significant between group differences in the cognitive assessments, within the assisted exercise group, significant effects were observed pre and post 6 weeks of exercise in the effort cognitive cluster. Based on Brown’s model, effort requires the cognitive capacity to sustain effort which is highly influential on processing speed, or cognitive efficiency; characteristics often reported as problematic in individuals with ADHD [12,52].
Verbal Fluency: The verbal fluency tasks assess the effort required to quickly produce a cognitive output response (e.g., semantic), as well as cognitive efficiency (e.g., phonemic). Semantic activation requires the capacity and effort to cognitively organize and filter words and concepts that are associated with the given category. If this process is impaired this can lead to associated word responses that may be related but do not fit the category. For example, if the category is animals, a correct response would be horse and an associated but incorrect response would be stable. Effort also involves the cognitive capacity to recognize and inhibit incorrect responses. Phonemic activation involves processing speed, or cognitive efficiency, which is better assessed by the phonemic task due to a greater capacity for related word sound association that does not require categorical filtering.
While the voluntary cycling group had only slight improvements in the semantic measure, the assisted cycling therapy group significantly improved in this task. Both groups improved on the phonemic task though no significant effect was found for either one. There is no research available that has specifically evaluated the effect of exercise on cognitive effort in ADHD populations but there is evidence of significant improvements in verbal fluency tasks following six months of aerobic exercise in populations with mild cognitive impairments [53]. Furthermore, this result is consistent with improvements in semantic language fluency which was reported following both Assisted and Voluntary cycling following an 8 week intervention in adolescents with DS [54].
Inhibition and set switching: The assisted exercise group demonstrated improvements on all of the tasks associated with the cognitive clusters focus, emotion and action, while the voluntary exercise group showed minimal improvement or no appreciable change. Deregulated attention capacity is one of the primary characteristics associated with ADHD. While most people with ADHD struggle with the inability to focus or sustain attention for long periods of time, there are often reports of states of hyper focus that also interfere with the ability to appropriately shift attention.
The Stroop test evaluated these cognitive abilities. The assisted exercise group demonstrated a slight trend for significance in focus and attention (p = 0.099), and a substantial trend toward significance in set-shifting (p = .060). The literature in this area does not specifically address ACT, although the findings are consistent with task improvement after bouts of acute aerobic exercise [53]. Studies specific to ACT in adolescents with ASD are consistent and reported improvements in the Stroop task after an acute ACT session but not after a VC session. Set switching ability as measured by the trail making test also increased following ACT but not VC or NC sessions in adolescents with ASD.
Dysregulated emotion has been identified as one of the cognitive deficits associated with ADHD [21]. However, the findings of this study failed to produce any appreciable changes within this cognitive domain for either group. This is likely due to the small sample size, but may also be explained by the researcher’s failure to control for the sub-types of ADHD. There is evidence suggesting dysregulated emotion is present more so in the combined inattentive/hyperactive presentation [39]. Lack of statistical power may also be due to the small population sample size evaluated for this study.
Self-regulation is another domain that has been reported to be deficient within the ADHD population. The findings of this study showed no statistical significance between groups or within groups for mean scores. However, when the scores were individually interpreted based on the parameters of the scale, two of the assisted exercise participants produced categorical scores which moved them into the moderate self-regulating capacity from a low self-regulating capacity, while the third participant moved from a moderate capacity to an intact capacity. Neither of the voluntary exercise participant’s pre/post evaluation scores differed, one initially scored and remained at a moderate capacity while the other scored and remained in the low capacity. Although no statistical differences in pre and post mean scores were observed, it is likely due to the small population sample size and the interpretation implicates the participants’ demonstrated noticeable changes in regulating capacity.
Motor Function Findings
In addition to executive function, motor function was evaluated through the Purdue Pegboard tasks for manual dexterity. Fine motor ability and coordination has been found to be significantly impaired in adolescent ADHD populations [17]. The Purdue Pegboard is a widely used assessment for the evaluation of fine motor ability through manual dexterity tasks involving the use of the dominant hand, non-dominant hand, and both hands combined. Each unimanual and bimanual task assesses how quickly and accurately the participant works with their hands while the assembly task assesses coordination.
There were no significant differences between exercise groups; however, the assisted exercise group improved on all manual dexterity tasks while the voluntary exercise group demonstrated minimal improvements. There was a significant change on the bimanual task within the assisted exercise group and the assembly task barely failed to attain statistical significance (p = .069). The findings are consistent with the research in persons with Down syndrome and Parkinson’s, other populations demonstrating neurocognitive motor impairments, after bouts of assisted exercise [33,34]. When you find improvements in the muscles that were not exercised (e.g., fine muscles), it can be interpreted that the changes were not physiological but are likely happening at the cortical level, which is consistent with our executive function findings.
CONCLUSION AND FUTURE DIRECTION
In conclusion, a six-week, three times per week assisted exercise intervention significantly improved cognitive capacities associated with executive function as well as bimanual dexterity. Evaluating the effects of assisted exercise is an innovative approach to assessing changes in executive and motor function among adult ADHD population and to the author’s knowledge is the first of its kind. Most research has been conducted in typical populations and in children with ADHD and commonly limited to acute bouts of voluntary aerobic exercise. While there were clear observable changes in some of the executive and motor function outcomes, studies with greater number of participants should be conducted in order to reinforce these findings. The results of this study are also limited to young adult females with ADHD and future studies involving other populations would be of great contribution, especially in children and adolescents. Since ADHD follows a lifelong trajectory of impairment, early intervention could greatly improve the quality of life for many individuals with ADHD well into adulthood.
Gaining a better understanding of the mechanisms involved with the observed changes is also of great importance. While it can by posited that neurocognitive changes are related to increases in production and upregulation of dopamine and BDNF, being able to measure these changes would provide greater insight into changing the developmental trajectory. While it is possible to evaluate these changes utilizing fMRI scans this component was beyond the scope of this study. It is evident that exercise produces changes in executive and motor functioning but in order for researchers to better observe and differentiate the changes observed between assisted and voluntary interventions, fMRI scans could be a useful instrument. The results from this study could be generalized to suggest that high rate exercise can help persons with ADHD function better in the classroom, at home and at work which is critical for their quality of life.
REFERENCES
- Polanczyk G, de Lima M, Horta B, Biederman J, Rohde L. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psych. 2007; 164: 942-948.
- Kessler R, Adler L, Barkley R, Biederman J, Conners C, Demler O, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication. Am J Psych.
- Farone SV, Biederman J, Mick E. The age dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psych Med. 2006; 36: 159-165
- Harpin VA. The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch Dis Child. 2005; 90: i2-i7.
- Pelham W E, Foster M, Robb JA. The economic impact of attention- deficit/hyperactivity disorder in children and adolescents. J Pedia Psych. 2007; 32: 711-727.
- Birnbaum HG, Kessler RC, Lowe SW, Secnik K, Greenberg PE, Leong SA, et al. Costs of attention deficit-hyperactivity disorder (ADHD) in the US: excess costs of persons with ADHD and their family members in 2000. Curr Med Res Opin. 2005; 21: 195-205.
- Frank-Briggs AI. Attention deficit hyperactivity disorder (ADHD). Journal of Pediatric Neurology. 2011; 9: 291-298.
- Hillman CH, Buck SM, Themanson JR, Pontifex MB, Castelli DM. Aerobic fitness and cognitive development: Event-related brain potential and task performance indices of executive control in preadolescent children. Dev Psychol. 2009; 45: 114-129.
- del Campo N, Chamberlain SR, Sahakian BJ, Robbins TW. The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Bio Psych. 2011; 69: e145-e157.
- Chandler C. The science of ADHD: A guide for parents and professionals.2011.
- Brown TE. Executive functions and attention deficit hyperactivity disorder: Implications of two conflicting views. Int J Disabil Dev Edu. 2007; 53: 35-46.
- Brown TE. A new understanding of ADHD in children and adults:Executive function impairments. 2013.
- Kelly K, Ramundo P. You mean I’m not lazy, stupid or crazy?!: the classic self-help book for adults with attention deficit disorder.1996.
- Hummer T, Kronenberger W, Wang Y, Dunn D, Mosier K, Kalnin A, et al. Executive functioning characteristics associated with ADHD comorbidity in adolescents with disruptive behavior disorders. J Abnorm Child Psychol. 2011; 39: 11-19.
- Berwid OG, Halperin JM. Emerging support for a role of exercise in attention-deficit/hyperactivity disorder intervention planning. Curr Psychiatry Rep. 2012; 14: 543-551.
- Sagvolden T, Johansen EB, Aase H, Russell VA. A dynamic developmental theory of attention-deficit/hyperactivity disorder (ADHD) predominantly hyperactive/impulsive and combined subtypes. Behav Brain Sci. 2005; 28: 397-418.
- Pitcher TM, Piek JP, Hay DA. Fine and gross motor ability in males with ADHD. Dev Med Child Neurol. 2003; 45: 525-535.
- Pitcher TM, Piek JP, Hay DA. Motor coordination and kinaesthesis in boys with attention deficit–hyperactivity disorder. Dev Med Child Neurol. 1999; 41: 159-165.
- Flapper BC, Houwen S, Schoemaker MM. Fine motor skills and effects of methylphenidate in children with attention-deficit–hyperactivity disorder and developmental coordination disorder. Dev Med Child Neurol.2006; 48: 165-169.
- Stray LL, Stray T, Iversen S, Ruud A, Ellertsen B, Tonnessen FE. The Motor Function Neurological Assessment (MFNU) as an indicator of motor function problems in boys with ADHD. Behav Brain Funct. 2009; 5: 22.
- Castellanos FX. Toward a pathophysiology of attention-deficit/ hyperactivint disorder. Clin Pediatr (Phila). 1997; 36: 381-393.
- Arnsten AFT. Toward a new understanding of attention-deficit hyperactivity disorder pathophysiology. CNS Drugs. 2009; 23: 33-41.
- Centers for Disease Control and Prevention (2008). Youth risk behavior surveillance system: Selected 2008 national health risk behaviors and health outcomes by sex. Retrieved from http://www. cdc. gov/ healthyyouth /yrbs/pdf/us_disparitysex_yrbs.pdf
- Tang A, Wanchoo SJ, Swann AC, Dafny N. Psychostimulant treatment for ADHD is modulated by prefrontal cortex manipulation. Brain Res Bull. 2009; 80: 353-358.
- Ribasés M, Hervás A, Ramos-Quiroga JA, Bosch R, Bielsa A, Gastaminza X, et al. Association study of 10 genes encoding neurotrophic factors and their receptors in adult and child attention-deficit/hyperactivity disorder. Biol psychiatry. 2008; 63: 935-945.
- Tsai SJ. Attention-deficit hyperactivity disorder may be associated with decreased central brain-derived neurotrophic factor activity: clinical and therapeutic implications. Med Hypotheses. 2007; 68: 896-899.
- Etnier JL, Nowell PM, Landers DM, Sibley BA. A meta-regression to examine the relationship between aerobic fitness and cognitive performance. Brain Res Rev. 2006; 52: 119-130.
- Verret C, Guay MC, Berthiaume C, Gardiner P, Beliveau L. A physical activity program improves behavior and cognitive functions in children with ADHD: An exploratory study. J Atten Disord. 2012; 16: 71-80.
- Dishman RK, Berthoud HR, Booth FW, Cotman CW, Edgerton VR, Fleshner MR, et al. Neurobiology of exercise. Neurobiol Exercis. 2006; 14: 345-356.
- Chang YK, Liu S, Yu HH, Lee YH. Effect of acute exercise on executive function in children with attention deficit hyperactivity disorder. Arch Clin Neuropsychol. 2012; 27: 225-237.
- Petzinger GM, Walsh JP, Akopian G, Hogg E, Abernathy A, Arevalo P, et al. Effects of treadmill exercise on dopaminergic transmission in the 1-methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine-lesioned mouse model of basal ganglia injury. J Neurosci. 2007; 27: 5291-5300.
- Schmolesky MT, Webb DL, Hansen RA. The effects of aerobic exercise intensity and duration on levels of brain-derived neurotrophic factor in healthy men. J Sports Sci Med. 2013; 12: 502-511.
- Alberts JL, Linder SM, Penko AL, Lowe MJ, Phillips M. It is not about the bike, it is about the pedaling: forced exercise and Parkinson’s disease. Exerc Sport Sci Rev. 2011; 39: 177-186.
- Ringenbach SD, Albert AR, Chen CCJJ, Alberts JL. Acute Bouts of Assisted Cycling Improves Cognitive and Upper Extremity Movement Functions in Adolescents With Down Syndrome. Intellect Dev Disabil. 2014; 52: 124-135.
- Culbertson WC, Zillmer EA. The construct validity of the Tower of London DX as a measure of the executive functioning of ADHD children. Assessment. 1998; 5: 215-226.
- Lansbergen MM, Kenemans JL, van Engeland H. Stroop interference and attention-deficit/hyperactivity disorder: a review and meta- analysis. Neuropsychology. 2007; 21: 251-262.
- Gualtieri CT, Johnson LG. Reliability and validity of a computerized neurocognitive test battery, CNS Vital Signs. Arch Clin Neuropsychol. 2006; 21: 623-643.
- Koziol LF, Stout CE. Use of a verbal fluency measure in understanding and evaluating ADHD as an executive function disorder. Percept Mot Skills. 1992; 75: 1187-1192.
- Wheeler Maedgen J, Carlson CL. Social functioning and emotional regulation in the attention deficit hyperactivity disorder subtypes. J Clin Child Psychol. 29: 30-42.
- Neumann A, van Lier PA, Gratz KL, Koot HM. Multidimensional assessment of emotion regulation difficulties in adolescents using the difficulties in emotion regulation scale. Assessment. 2010; 17: 138-149.
- Klingberg T, Forssberg H, Westerberg H. Training of working memory in children with ADHD. J Clin Exp Neuropsychol. 2002; 24: 781-791.
- Miller WR, Brown JM. Self-regulation as a conceptual basis for the prevention and treatment of addictive behaviours. Self-control and the addictive behaviours, 3-79.
- CAASA. Self-regulation questionnaire. Assessment Instruments. 2006.
- Riccio CA, Wolfe ME, Romine C, Davis B, Sullivan JR. The Tower of London and neuropsychological assessment of ADHD in adults. Arch Clin Neuropsychol. 2004; 19: 661-671.
- Mitchell JT. Cognitive-Behavioral Therapy for Adult ADHD: Targeting Executive Dysfunction. Arch Clini Neuropsycho. 2012; 27: 934-935.
- Chang YK, Tsai CL, Hung TM, So EC, Chen FT, Etnier JL. Effects of acute exercise on executive function: a study with a tower of london task. J Sport Exerc Psychol. 2011; 33: 847-865.
- Holzapfel SD, Ringenbach SDR, Mulvey GM, Sandoval-Menendez AM, Birchfield N, Tahiliani SR. Differential effects of Assisted Cycling Therapy (ACT) on short-term and working memory of adolescents with Down syndrome. J Cogn Psychol. 2016; 28: 990-1003.
- Fassbender C, Cortes CR, Tagamets MA, Windsor TA, Reeves GM, Gullapalli R, et al. Working memory in attention deficit/hyperactivity disorder is characterized by a lack of specialization of brain function. PloS One. 2011; 6: e27240.
- Pontifex M, Hillman C, Fernhall B, Thompson K, Valentini T. The effect of acute aerobic and resistance exercise on working memory. Med Sci Sports Exerc. 2009; 41: 927-934.
- Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart: exercise effects on brain and cognition. Nat Rev Neurosci. 2008; 9: 58- 65.
- Ringenbach SDR, Holzapfel SD, Mulvey GM, Jimenez A, Benson A, Richter M. The effects of Assisted Cycling Therapy (ACT) and voluntary cycling on reaction time and measures of executive function in adolescents with Down syndrome. J Intellect Disabil Res. 2016; 60: 1073-1085.
- Abreu N, Argollo N, Oliveira F, Cardoso AL, Bueno JL, Xavier GF. Semantic and phonologic verbal fluency tests for adolescents with ADHD. Clin. Neuropsychiatry. 2013; 10: 63-71.
- Baker LD, Frank LL, Foster-Schubert K, Green PS, Wilkinson CW, McTiernan A, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol. 2010; 67: 71-79.
- Ringenbach SDR, Holzapfel SD, Mulvey GM, Pandya S. Assisted Cycle Therapy (ACT) for persons with Down syndrome: Implications for improvements in cognitive functioning. Health Problems in Down Syndrome, InTech. 2015; 70-84.








































































































































