Hydrogel for Treatment of a Symptomatic Trigeminal Neuroma: A Case Report
- 1. Department of Surgery, University of Texas Southwestern Medical Center, USA
- 2. Department of Surgery and Neurology, University of Texas Southwestern Medical Center, USA
Abstract
Trigeminal nerve injuries may cause significant functional impairments. When trigeminal nerve injuries require surgical intervention, microsurgical repair has proven to be a reliable means of achieving functional sensory recovery. However, a considerable challenge arises when the distal nerve stump is unidentifiable or severely atrophied, inhibiting microsurgical repair. Recently, a bioresorbable hydrogel nerve cap has received Food and Drug Administration approval as a de novo device for the prevention of peripheral nerve neuromas. The purpose of this case report was to determine if the hydrogel nerve cap is a feasible option for the treatment of trigeminal neuroma when microsurgical repair is not possible.
Keywords
• Trigeminal nerve; Neuroma; Nerve cap; Hydrogel
Citation
Neal TW, Zuniga JR (2026) Hydrogel for Treatment of a Symptomatic Trigeminal Neuroma: A Case Report. J Neurol Disord Stroke 13(1): 1248.
INTRODUCTION
Trigeminal nerve injuries may cause significant functional impairments, including pain, unintentional tongue and lip chewing, drooling while eating or drinking, and difficulty speaking. The branches of the trigeminal nerve usually affected are the inferior alveolar nerve (IAN) and the lingual nerve (LN). These injuries are most commonly caused by third molar extraction, orthognathic surgery, mandibular trauma, dental implant placement, local anesthesia injection, endodontic therapy, and pathology resection [1]. Depending on the mechanism and severity of injury, most injured IANs and LNs recover spontaneously [2].
When trigeminal nerve injuries require surgical intervention, microsurgical repair has proven to be a reliable means of achieving functional sensory recovery [3,4]. Microsurgical repair can be completed with various techniques, including direct neurorrhaphy, connector-assisted neurorrhaphy, autograft reconstruction, and allograft reconstruction. Often, there are viable proximal and distal nerve stumps to perform these techniques to restore function. A considerable challenge arises when the distal nerve stump is unidentifiable or severely atrophied, inhibiting microsurgical repair. Current treatment strategies include burying the proximal nerve stump in muscle, using a porcine small intestine submucosa nerve cap, and performing distal neurorrhaphy into the residual buccal soft tissue. Recently, a bioresorbable hydrogel nerve cap has received Food and Drug Administration approval as a de novo device for the prevention of peripheral nerve neuromas. The purpose of this case report was to determine if the hydrogel nerve cap is a feasible option for the treatment of trigeminal neuroma when microsurgical repair is not possible.
CASE PRESENTATION
A 77-year-old female presented with a chief complaint of neurosensory disturbance and pain in the right mental nerve distribution 10 months after mandibular dental implant placement. Her past medical history was noncontributory to the chief complaint. Cone beam computed tomography scan revealed dental implants placed anterior to the mental foramen without impingement. However, there was severe atrophy of the mandible, with the mental foramen located at the superior mandibular alveolus. Clinical neurosensory testing was completed as previously described [6]. There was a loss of two-point discrimination and directional sensation in the right mental nerve distribution. Additionally, there was increased contact and pain thresholds compared to the left mental nerve distribution, which served as the control side. Pain was elicited with palpation, indicating a trigger, but no neuropathic pain was elicited on exam. These clinical findings indicated a sensory function of S2 on the Medical Research Council Scale (some superficial pain and touch sensation).
The patient was taken to the operating room for excision of suspected neuroma and neurorrhaphy. Intraoperative findings revealed a Sunderland class V injury of the right inferior alveolar nerve with a 6-millimeter amputation neuroma. The neuroma was excised and connector assisted neurorrhaphy was performed. The patient had a symptom free period; however, she did not present for follow up until 15-months post-surgery with complaints of a small mass that is painful to palpation. Clinical exam revealed no change in neurosensory testing, and a persistent trigger with a small palpable mass at the mental foramen. Magnetic resonance neurography imaging revealed a recurrent 5-millimeter neuroma of the right mental nerve (Figure 1).

Figure 1 Coronal view of magnetic resonance neurography 3-dimensional maximum intensity projections 15 months after neuroma excision and connector assisted neurorrhaphy. There is recurrent neuroma formation of the right inferior alveolar nerve (arrow).
She was then taken for a second procedure to excise the recurrent neuroma. Intraoperative findings revealed a large amputation neuroma of the right mental nerve with atrophy of the distal nerve branches (Figure 2).

Figure 2 A) Intraoperative view of the right recurrent mental nerve neuroma (arrow). B) Intraoperative view of right mental nerve following resection of the neuroma with posterior mandible decortication for access.
Since neurorrhaphy was not feasible, hydrogel nerve cap (allay Nerve Cap, Tulavi Therapeutics, Los Gatos, CA) was used. The cut proximal nerve stump was placed in the silicone mold and the hydrogel was applied. The mold was then removed after polymerization, and the procedure was completed (Figure 3).

Figure 3 A) Proximal nerve stump placed in the silicone former. B) Hydrogel placed and polymerizing. C) Polymerized hydrogel nerve cap completed.
A month following nerve cap placement, the patient developed a pathologic fracture of the right body of the mandible that required open reduction and internal fixation, allowing for direct visualization of the nerve cap. Intraoperative findings revealed an intact hydrogel nerve cap without recurrent neuroma formation (Figure 4).
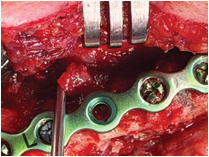
Figure 4 Intraoperative view 1 month after placement of hydrogel nerve cap. The nerve cap is intact without recurrent neuroma formation.
Four months following placement of the hdxydrogel nerve cap, the patient was pain free with no clinical evidence of neuroma formation.
DISCUSSION
The present case shows that hydrogel nerve cap is a feasible treatment for a trigeminal neuroma when microsurgical repair is not possible. Under direct intraoperative visualization of the site 1-month post hydrogel placement, no neuroma recurrence was observed. Additionally, 4 months after placement of the hydrogel nerve cap, there were no clinical symptoms of neuroma recurrence.
The hydrogel nerve cap is composed of polyethylene glycol and water. The silicone former allows for application around the circumference of a transected nerve, creating a barrier that prevents axonal escape and tethering to surrounding tissues. Preventing axonal outgrowth leads to distal Schwann cell apoptosis and the exhaustion of nerve regeneration. After polymerization, the nerve cap is soft and elastic and completely resorbs within 8 months.
There are few reports detailing the management of trigeminal nerve injuries that cannot be reconstructed and require proximal stump relocation or capping. Bellamy et al. reported a case of a patient who developed chronic tongue pain after excision of a benign mass. A large lingual nerve amputation neuroma was found. The neuroma was excised, and the proximal nerve stump was buried in the mylohyoid muscle with reported resolution of preoperative pain symptoms [7]. Watson et al reported a case of a 14-year-old who sustained a traumatic injury to the right infraorbital nerve. The patient developed causalgia that did not respond to medical treatment. No neuroma was identified, but the contused portion of the nerve was excised, and the proximal stump was buried in buccal fat with resolution of preoperative pain symptoms [8]. Although no results were reported, Miloro suggests that distal neurorrhaphy into the residual buccal soft tissues will lead to axonal sprouting and sensory reinnervation of the lower lip and chin [9]. The basis of this suggestion was the results of targeted muscle reinnervation with motor nerves of the upper or lower extremity. A difficulty with this technique is the lack of expendable facial motor nerve branches available for coaptation.
Ostrowski et al., used hydrogel nerve cap for the treatment and prevention of 23 nerves of the upper and lower extremities. Of the 10 patients who received hydrogel treatment to prevent neuroma formation after nerve transection, none developed symptomatic neuromas. Two patients with established symptomatic neuromas underwent neuroma excision and placement of hydrogel nerve cap. Both patients experienced a significant decrease in postoperative visual analog scale score during the study period [10]. The authors reported an average time of 55 seconds to apply the hydrogel nerve cap. The present case utilizes the device in the oral cavity, a small surgical field with limited access. Our experience was similar, with an application time of less than 2 minutes.
In the surgical management of trigeminal nerve injuries, the goal is the return of functional sensation. It is rare that repair or reconstruction is not possible. Therefore, the hydrogel nerve cap has limited use for the trigeminal nerve surgeon. However, in specific cases such as the one presented, the hydrogel nerve cap is a feasible treatment option. The device is easy-to-use with the distinct advantage of suture less application.
Conflict of Interest
JRZ is a consultant for Axogen Inc. TWN has no disclosures to report.
REFERENCES
- Tay AB, Zuniga JR. Clinical characteristics of trigeminal nerve injury referrals to a university centre. 2007; 36: 922-927.
- Zuniga JR. Sensory outcomes after reconstruction of lingual and inferior alveolar nerve discontinuities using processed nerve allograft-a case series. 2015; 73: 734-744.
- Pogrel MA. The results of microneurosurgery of the inferior alveolar and lingual nerve. 2002; 60: 485-489.
- Jacobs T, Mohammed S, Ziccardi V. Assessing the efficacy of allogeneic nerve grafts in trigeminal nerve repair: A systematic review. 2024; 82: 294-305.
- Miloro M. What do I do if there is no distal nerve stump for inferior alveolar nerve reconstruction? 2023; 81: 1443-1446.
- Zuniga JR, Essick GK. A contemporary approach to the clinical evaluation of trigeminal nerve injuries. 2011; 23: 353-367.
- Bellamy JL, Steinbacher DM, Debrux JC, Magarakis M, Rosson GD. Treatment of recurrent lingual nerve end-neuroma: A case report. 2013; 33: 575-577.
- Watson CP, Stinson JN, Dostrovsky JO, Hawkins C, Rutka J, Forrest C. Nerve resection and re-location may relieve causalgia: A case report. 2007; 132: 211-217.
- Miloro M. What do I do if there is no distal nerve stump for inferior alveolar nerve reconstruction? 2023; 81: 1443-1446.
- Ostrowski P, Deng I, Kobraei EM. A novel hydrogel for treatment and prevention of symptomatic neuroma: Early clinical experience. 2025; 13: e7339.








































































































































