An Unusual Presentation of Neuroblastoma in an Infant
- 1. Department of Pediatric Neurology, Women and Children’s Hospital of Buffalo, State University of New York at Buffalo, USA
- 2. Department of Pathology, Women and Children’s Hospital of Buffalo, State University of New York at Buffalo, USA
- 3. Liaqat University of Medical and Health Sciences, Jamshoro, Pakistan
Citation
Farooq O, Khan AR, Kirmani A, Kerr SL (2013) An Unusual Presentation of Neuroblastoma in an Infant. J Neurol Transl Neurosci 1(3): 1022.
CLINICAL IMAGE
A 7 week old female with “congenital torticollis,” was referred for neurological consultation for persistent decreased movements of her arms. The mother described noticeably floppy arms and a weak neck with her head constantly resting on her left shoulder. Neurological examination revealed decreased tone and strength in the proximal upper extremities bilaterally, with fisting of the hands and nearly absent deep tendon reflexes. Examination of the lower extremities was normal. An MRI of the cervical spine revealed an intraspinal extradural mass extending from C4-T1 (Figure 1a and 1b).
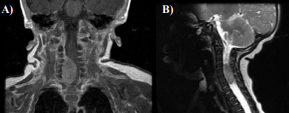
Figure 1 MRI of the cervical spine revealed an intraspinal extradural mass extending from C4-T1 (panel A, T1 with contrast, coronal view; panel B, T2 sagittal view). This mass measures approximately 14 x 11 mm by approximately 24 mm craniocaudad. There is mass-effect on the spinal cord which is displaced to the left. The mass extends into several of the right neural foramina. The mass has mildly increased signal on T2-weighted images and intermediate signal on T1-weighted images and shows some contrast enhancement.
A prompt surgical resection was performed and histopathological analysis was consistent with neuroblastoma (Figure 2).
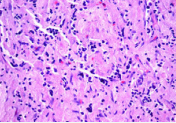
Figure 2 Photomicrograph showing schwannian stroma-poor neuroblastoma (poorly-differentiated neuroblastoma), with intermediate Mitotic Karyorrhectic Index (MKI), favorable histology (H&E stain x 400). The majority of the tumor cells are undifferentiated neuroblasts (thick arrow). The differentiating cells which constitute less than 5% are highlighted by the vertical arrow. A Mitosis is seen in the right upper corner (thin arrow)
Neuroblastomas are embryonal malignancies derived from primordial neural crest cells which subsequently develop into sympathetic ganglia and the adrenal medulla. As a result, neuroblastomas can develop anywhere along the sympathetic chain from the neck to the groin. It is the third most common malignancy in children after leukemia and primary CNS brain tumors and the most common extra cranial solid tumor of infancy [1,2].
Primary lesions are most commonly found in the abdomen; however they can occur anywhere along the sympathetic plexus in roughly 25% of cases and specifically in the neck in about 5% [3]. A paraspinal mass at any level can cause compression of the spinal cord and present with neurological symptoms, limb weakness, and bladder or bowel dysfunction. The presence of these symptoms requires urgent investigation and intervention [4,5].
Our patient presented with a solitary cervical spine lesion, causing her to have a unilateral head lag. Although a paraspinal presentation of neuroblastoma is less frequently encountered, it can easily be misdiagnosed as congenital torticollis. Upon performing a thorough neurological examination, the findings did not correlate with congenital torticollis, and instead suggested cervical cord pathology. This ultimately led to neuroimaging which revealed the correct diagnosis. Therefore congenital torticollis should only be diagnosed in the absence of localizing clinical features.
Neuroblastoma should be considered in the differential diagnosis of a child with an abdominal or paraspinal mass. This underlies the need for prompt neuroimaging in infants who present with neck tone abnormalities (hypo/hypertonia), unilateral or bilateral limb weakness and/or abnormal deep tendon reflexes. Infants with neuroblastoma tend to have a better prognosis than older children. Our patient continues to do well post-resection (Figure 3).
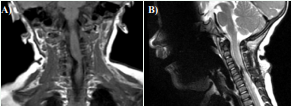
Figure 3 Follow up MRI performed 2 months post resection (panel A, T1 coronal view; panel B, T2 sagittal view). There is still mass-effect on the spinal cord with deviation of the cord to the left. This is most pronounced at C5-C6. There is continued evidence of increased soft tissue density in the right neural foramen at C5-C6 and to a lesser degree at C6-C7. On both the sagittal and coronal images the abnormality is centered at C5-C6.







































































































































{kind=link}