Determining the Long-Term Use of Antiepileptic Medications in Patients with Posterior Reversible Encephalopathy Syndrome: A Case Report and Review of the Literature
- 1. Department of Neurology, University of Florida Health Sciences Center Jacksonville, USA
Abstract
Purpose: To discuss the long-term use of antiepileptic drugs (AED) in patients with posterior reversible encephalopathy syndrome (PRES).
Method/Results: We present a case report of an individual who presents with mental status changes and who developed seizures as the early presentation of PRES. The patient was treated with phenytoin. More than half a year later, both EEG and neuroimaging studies reverted to normal. However, the patient continued to have persistently elevated blood pressure. Because of this, AED therapy was continued.
Conclusion: The case illustrates a dilemma encountered in the management of patients with PRES. A literature search review reveals a lack of information on the use of AEDs in patients with a previous history of PRES who continue to have elevated blood pressure. Future studies should determine whether successful management of blood pressure in this population of patients should be a prerequisite prior to withdrawal of AED therapy.
Keywords
• Antiepileptic drugs
• Epilepsy: hypertension
• Posterior reversible encephalopathy syndrome
• Seizures
Citation
Rodríguez Rosario LB, Bautista RED (2013) Determining the Long-Term Use of Antiepileptic Medications in Patients with Posterior Reversible Encephalopathy Syndrome: A Case Report and Review of the Literature. J Neurol Transl Neurosci 1: 1014.
INTRODUCTION
Posterior reversible encephalopathy syndrome (PRES) is a clinical and radiological entity with symptoms that include headaches, confusion, seizures, and visual loss. It may occur due to a number of causes, such as malignant hypertension, eclampsia, and immunosuppressive drugs. Magnetic resonance imaging (MRI) of the brain demonstrates areas of vasogenic edema most commonly in the parieto-occipital lobes although other areas may be involved. MRI findings tend to resolve after a period of time, however case reports have suggested the possibility of PRES recurrence and neurological sequelae such as chronic epilepsy [1]. As illustrated in this case study, one issue that remains unresolved is whether patients who have experienced seizures due to PRES should be maintained on chronic antiepileptic drug (AED) therapy if they continue to experience uncontrolled hypertension despite resolution of neuroimaging abnormalities.
CASE REPORT
A 51-year-old female presented to emergency department (ED) with a one day history of altered mental status after being found by family members to be confused and disoriented with slurring of speech. On arrival to the ED, blood pressure was 219/121. The patient was lethargic and oriented to person only and was not able to follow commands consistently. Pupils were equally reactive to light and no craniofacial asymmetries were noted. The patient was able to move all extremities symmetrically and was able to withdraw to noxious stimuli. There was increased tone and hyperreflexia in her upper extremities bilaterally but normal tone and normal reflexes in her lower extremities. Plantar response was equivocal bilaterally.
Her past medical history was significant for hypertension, diabetes mellitus, gout, asthma, perforated bowel status post colostomy, and an enterocolovaginal fistula. There was no prior history of seizures, history of head trauma, meningitis, encephalitis, staring spells, or periods of confusion prior to this episode. There was no family history of seizures.
A complete blood count and basic metabolic panel was normal. An initial computerized tomography scan of the head showed diffuse cerebral atrophy. A lumbar puncture was performed and was also unremarkable.
Because of the elevated blood pressure, 20 mg intravenous (IV) of labetalol was administered. The patient had a witnessed generalized tonic-clonic seizure in the ED that resolved only after administration of 1mg of IV lorazepam and phenytoin 1 gm IV. The patient was then intubated and maintained on phenytoin 100 mg IV every 8 hours.
A MRI of the brain demonstrated multifocal areas of T2 hyperintensities predominantly over both parieto-occipital regions, compatible with posterior reversible encephalopathy syndrome (PRES) (Figure 1).
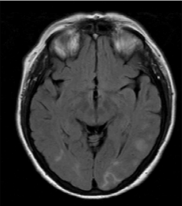
Figure 1 Magnetic Resonance Imaging shows increased T2 signals over the parieto-occipital regions consistent with a diagnosis of posterior reversible encephalopathy syndrome.
Maintenance antihypertensive medications resulted in adequate control of blood pressure. A repeat EEG the following day showed diffuse beta and delta activity with no evidence of electrographic seizure activity. The patient was subsequently extubated and discharged after 2 days on doxazosin, minoxidil, lisinopril, atenolol, and phenytoin .
On outpatient follow-up, no further seizures occurred. A repeat MRI of the head was performed 6 months after discharge and showed resolution of PRES. A routine EEG performed 8 months after discharge was normal. However, the patient continued to have poor blood pressure control (164/79 mmHg). Because of this, we opted to maintain the patient on AED therapy.
DISCUSSION
Posterior reversible encephalopathy syndrome (PRES) has been well reported in the literature. Although hypertension is one of the etiologies described in the literature as the cause of PRES, the exact pathogenesis remains unclear. Seizures and altered mental status are a common clinical presentation among patients with posterior reversible encephalopathy [2]. Seizures are usually focal with secondary generalization, can vary in number, and are usually of limited duration [3,4].
Wagner and colleagues [3] studied PRES in the setting of eclampsia and noted that the blood pressure levels were lower than those reported in cases of PRES secondary to hypertension with a mean peak systolic blood pressure of 173 mmHg. This study suggests that pregnant patients need to have better control of their blood pressure as minimal increases may be sufficient to cause the development of PRES.
Li and colleagues [5] studied the clinical profile and factors that predicted recurrence in patients who had PRES. Most of the patients in that study had confusion followed by abrupt neurologic deterioration that was heralded by a seizure. One third of patients progressed into status epilepticus or coma requiring intubation and mechanical ventilation as in our case. More importantly, 14% of patients had recurrence of PRES and poorly controlled hypertension was the main etiology that determined recurrence.
Although by definition PRES findings resolves after time, Komur and colleagues [6] reported a case of a child with hypertension due to end stage renal disease who had recurrent PRES and findings on MRI persisting as encephalomalacia. In a long term follow-up study by Roth and Ferbert [7], a total of 25 patients with PRES were identified. Eighty-eight percent had generalized seizures but no patient developed status epilepticus. Two patients had recurrence of PRES related to hypertension and the calculated incidence for recurrence was 8%. Etiologies of PRES were mostly due to hypertensive crisis and eclampsia though other causes such as chemotherapy, pancreatitis and infectious process were identified. The mean blood pressure was 170/98 mmHg and 4 patients had chronic hypertension before their first episode of PRES [7]. It is not uncommon to see a systolic blood pressure of 180 mmHg on a daily basis but the incidence for PRES is significantly less. Rabinstein and colleagues [8] compared the blood pressure of those who developed PRES versus controlled patients matched for age, gender, and history of hypertension, and concluded that although acute hypertension is frequent in patients with PRES, blood pressure fluctuations were not more common when compared to controls. This raises the question about what other factors might be contributing to the development of PRES.
Although long-term prognosis is generally favorable, delayed recognition of PRES can result in permanent brain damage. There have been reported cases of fulminant and fatal presentations in situations where the diagnosis and treatment was delayed, resulting in permanent ischemia and intracerebral hemorrhage [9,10].
Chemotherapy agents are also described as a cause for PRES in the literature and often occur in patients on chemotherapy who develop sudden rises in blood pressure. The management of those patients includes the discontinuation of the offending agent, use of AEDs, and aggressive blood pressure management [10]. There are no established guidelines for the optimal degree of blood pressure lowering in PRES. An initial 20-25% reduction of the mean arterial pressure has been established as a reasonable goal for immediate reduction of blood pressure in patients with hypertensive crisis [2]. Further optimization of blood pressure then depends on the patient’s clinical status and other comorbidities.
As this case report indicates, data on the long-term use of AEDs has not been established in patients who have persistently elevated blood pressures, even if neuroimaging and EEG findings have normalized. This is specifically pertinent in our patient who developed seizures during the early presentation of PRES. There is a report of breakthrough seizures following the initial presentation of status epilepticus in a child with PRES [11]. It remains unclear whether seizures as one of the initial presentation of PRES predict future risk for seizures. In our case, it was felt that because our patient experienced seizures and her blood pressure remained poorly controlled, AEDs ought to be continued.







































































































































{kind=link}