External Hydrocephalus without Ventriculomegaly Following Endovascular Treatment of Subarachnoid Hemorrhage
- 1. Department of Neurosciences, St. Joseph Medical Center, USA
- 2. Department of Electrical Engineering and Computer Science, Vanderbilt University, USA
Abstract
External hydrocephalus occurs frequently with ventriculomegaly and refers to extra axial fluid collections observed after subarachnoid hemorrhage. Early symptomatic external hydrocephalus without ventriculomegaly following endovascular coil embolization of a ruptured aneurysm has not been previously reported.
Keywords
• Cerebral aneurysm
• Subarachnoid hemorrhage
Citation
Ajeet G, Aniruddh S (2016) External Hydrocephalus without Ventriculomegaly Following Endovascular Treatment of Subarachnoid Hemorrhage. J Neurol Transl Neurosci 4(2): 1068
ABBREVIATIONS
CSF: Cerebrospinal Fluid; SAH: Subarachnoid Hemorrhage
INTRODUCTION
External hydrocephalus refers to extra axial fluid collections observed after subarachnoid hemorrhage, and is frequently identified with ventriculomegaly. External hydrocephalus without ventriculomegaly has been identified in the context of surgical clipping of ruptured aneurysms. Symptomatic external hydrocephalus without ventriculomegaly following endovascular coiling of a ruptured aneurysm has not been reported.
CASE PRESENTATION
A 57-year-old male presented with a Hunt and Hess grade 2 and Fischer grade 3 subarachnoid hemorrhage (SAH) (Figure 1).
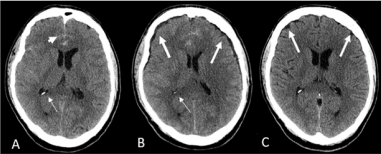
Figure 1 Axial non contrast head CT shows (A) subarachnoid hemorrhage (short arrow) without ventriculomegaly (thin arrow). (B) Bi-frontal extra axial fluid collections or external hydrocephalus (thick arrows) without ventriculomegaly (thin arrow). (C) Resolved extra axial collections (thickarrows) and subarachnoid hemorrhage.
Coil embolization of a 6 mm anterior communicating artery aneurysm was performed without incident. Two days post ictus, the patient complained of a worsening headache with no accompanying neurologic deficit. A non-contrast head CT demonstrated CSF attenuating prominence of the bilateral frontal extra axial spaces without associated mass effect or ventriculomegaly. The patient’s pain was managed with opiates and he was closely monitored in the intensive care unit. He remained hemodynamically stable with no neurologic change. A head CT obtained on day 7 post ictus revealed complete resolution of the extra axial fluid collections and SAH. The patient was discharged on day 14, with resolution of his headache and without a neurologic deficit.
DISCUSSION
External hydrocephalus or extra axial fluid collections are frequently identified by accompanying ventriculomegaly [1]. Such fluid collections are observed after surgical or endovascular treatment of ruptured aneurysms, hypothesized to be consequent to interruption of CSF flow [2,3]. After surgical treatment of ruptured aneurysms, external hydrocephalus without ventriculolmegaly has however been described [3]. A case report identifying early external hydrocephalus without ventriculomegaly following endovascular coiling of a ruptured cerebral aneurysm has not been reported.
External hydrocephalus and subdural hygromas are difficult to differentiate. A study by Alotaibi et al. identified spontaneous subdural fluid collection following SAH, noting the concurrent presence of external hydrocephalus and ventriculomegaly [2]. This is crucial in discriminating external hydrocephalus from subdural hygromas. Subdural hygromas may occur in the absence of CSF flow interruption after mild head trauma [1]. Atraumatic subdural hygroma results from tearing of the arachnoid membrane and subsequent CSF influx [4]. External hydrocephalus after SAH is caused by hemorrhage into the subarachnoid space and ventricles, with subsequent CSF flow obstruction [5]. Post-traumatic subdural hygromas often develop into subdural hematomas [6]. Similar studies on post-SAH extra axial collections, have not reported conversion to subdural hematomas, further differentiating the two as separate clinical entities.
CONCLUSION
External hydrocephalus and subdural hygroma differ in treatment. Ventricular shunt placement effectively resolves external hydrocephalus and improves clinical outcomes. Shunting potentially exacerbates hygromas [7]. Conservative expectant management of external hydrocephalus without ventriculomegaly is a feasible option, if no associated neurologic deficit is identified. With imaging resolution of a subarachnoid hemorrhage related extra axial collection, a retrospective confirmation of an external hydrocephalus can be made, differentiating it from a hygroma.









































































































































{kind=link}