Secondary Shoulder Impingement Caused by Combined Spinal Accessory Nerve and Dorsal Scapular Nerve Palsy
- 1. Department of Orthopedics and Traumatology, Istanbul Bilim University, Turkey
- 2. Department of Orthopedics and Traumatology, Fatih Medical Park Hospital, Turkey
- 3. Department of Plastic and Reconstructive Surgery, Istanbul Bilim University, Turkey
Abstract
Introduction: Subacromial impingement syndrome (SAIS) is the most common disorder of the shoulder, and may seldom be secondary to scapulothoracic muscle weakness due to the injury of the nerves innervating these muscles. Spinal accessory nerve (SAN) lesions may coexist with dorsal scapular nerve (DSN) injuries, which are commonly misdiagnosed. This is the first report in the literature that describes simultaneous palsies of SAN and DSN.
Case presentation: A 26-year-old Caucasian male with asymmetric shoulders reported pain when abducting his right arm to shoulder level and a decreased range of movement in right shoulder after two weeks of an accident carrying a heavy air-conditioner on his right shoulder. His right trapezius muscle showed signs of atrophy, with loss of the nuchal ridge and droping of the right shoulder girdle, internal rotation of the shoulder, and a wide area of dysesthesia on the neck. He was unable to shrug the effected shoulder, with presence of subacromial impingement signs. Plain radiographs and MRI scans were revealed no abnormalities. SAN and DSN palsy caused by compression of the posterior cervical triangle were diagnosed.
Conclusions: Nerve injury should be considered in the differential diagnosis of impingement syndrome. The DSN and SAN are in close proximity at the posterior cervical triangle, and when there is SAN palsy, an accompanying DSN injury should be ruled out due to the close proximity of these two nerves. This knowledge is important for planning of physical therapy and during follow-ups and also for the surgical exploration if it is necessary.
Keywords
• Secondary impingement
• Spinal accessory nerve palsy
• Dorsal scapular nerve
• Nerve palsy
Citation
Aksu N, Abay B, Aksu T, Tuncer S (2016) Secondary Shoulder Impingement Caused by Combined Spinal Accessory Nerve and Dorsal Scapular Nerve Palsy. J Neurol Transl Neurosci 4(3): 1069
ABBREVIATIONS
SAIS: Subacromial Impingment Syndrome; SAN: Spinal Accessory Nerve; DSN: Dorsal Scapular Nerve; MRI: Magnetic Resonance Imaging; ROM: Range of Motion.
INTRODUCTION
Subacromial impingement syndrome (SAIS) of the shoulder is the most common disorder of the shoulder. This disorder can present in many forms, ranging from inflammation to degeneration of the bursa and rotator cuff tendons of the subacromial space, and may lead to a full-thickness tear of the rotator cuff tendons and degenerative joint disease of the joints of the shoulder girdle. Shoulder impingement has been classified into primary and secondary types. Primary impingement occurs with specific alterations in the shape of the acromion process while secondary impingement occurs without these changes. Several biomechanical factors can contribute to secondary impingement, including rotator cuff muscle weakness, joint capsule restriction and dysfunctional coordination of scapulothoracic muscles. Scapulothoracic muscle weakness is another factor that can contribute to impingement [1,2]. When there are impingement signs on physical examination, and there are no signs of primary impingement on plain radiographs and MRI, then possible causes of secondary impingement, including scapulathoracic dysfunction due to paralysis of the trapezius muscle innervated by the spinal accessory nerve, levator scapula and rhomboid muscles innervated by the dorsal scapular nerve and serratus anterior muscle innervated by the long thoracic nerve should be sought.
The dorsal scapular nerve (DSN) accompanies the spinal accessory nerve (SAN) in the posterior cervical triangle. Spinal accessory nerve palsy resulting from compression of the posterior cervical triangle may be accompanied by DSN palsy, which may be missed. We report a rare secondary shoulder impingement caused by combined neuropathy of both the spinal accessory and dorsal scapular nerves secondary to compression of the posterior cervical triangle.
CASE PRESENTATION
In the outpatient department, we examined a 26-year-old Caucasian male with asymmetric shoulders who reported pain when abducting his right arm to shoulder level and a decreased range of movement in the right arm. Two weeks earlier, he had been carrying a heavy air-conditioner on his right shoulder when the load slid over his shoulder and fell.
His right trapezius muscle showed signs of atrophy, with loss of the nuchal ridge and dropping of the right shoulder girdle, internal rotation of the shoulder, and a wide area of dysesthesia on the neck. His right scapula was displaced laterally, rotated downward and outward. The supraclavicular fossa was deepened as results of trapezius atrophy (Figure 1)
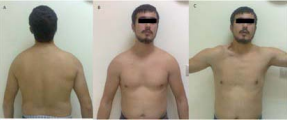
Figure 1 A 26-year-old man with both spinal accessory nerve and dorsal scapular nerve palsy caused by compression of the posterior cervical triangle. A) and B) His shoulders are asymmetrical, given the drooping of the right shoulder girdle. C) The restricted right shoulder, showing the deepened supraclavicular fossa on active abduction. He reported pain when abducting his right arm to shoulder level and a decreased range of movement in the arm.
Active movements were restricted to 90° in abduction and 160° in flexion. He was unable to shrug the effected shoulder, with presence of subacromial impingement signs.
There was no weakness of the sternocleidomastoid muscle, yet there was winging of the scapula noticed when the patient was told to push against the wall. He had a full range of passive movements and an unremarkable neurological examination. Plain radiographs and MRI scans of the cervical spine and shoulder revealed no abnormalities. Electromyography revealed a delay in the motor potentials of the right trapezius, levator scapula, and major and minor rhomboids that was consistent with neuropathic changes, and there were no findings of radiculopathy. Traumatic SAN palsy (sparing fibers to the sternocleidomastoid) and DSN palsy (with lesions at brachial C5 and cervival C3, C4) of the right shoulder were diagnosed.
The patient described intense pain, which was initially controlled with 50 mg Tramadol tablets twice a day for 10 days, and then by tenoxicam 20 mg once a day. Vitamin B1-B6 complex vitamin tablets (250 mg) were given twice a day. The patient was given Codman’s pendulum exercises (5 sets per day for 5 minutes for each set) on the affected shoulder. Then, a physical therapy and rehabilitation program consisting of active and passive ROM of the right shoulder and the neck, muscle-strengthening (mainly scapula stabilizing muscles, rhomboid and levator scapula) exercises were applied. The patient exercised 3 days a week in the clinic for 1 month. This was followed by a home exercise program. In the last follow- up on the third month after the injury, the patient recovered completely. There was no scapular winging, and physical examination was normal.
DISCUSSION
The scapulathoracic muscles that stabilize and rotate the scapula are the trapezius, rhomboids, levator scapulae, and the serratus anterior muscle. The rotations at the glenohumeral and scapulothoracic articulations are largely responsible for humeral abduction and flexion. The overall ratio of glenohumeral to scapulothoracic rotation is 2:1 throughout the full range of elevation.

Figure 2 Active range of motion in his right arm was restricted to 90° in abduction (A) and to 160° in flexion (B). (Photos used with the permission of the patient).
At less than 100° humeral elevation, the force of the upper trapezius and levator scapula fibers counteracts the lateral pull of the deltoid and upwardly rotates the acromion. Simultaneously the serratus anterior protracts the scapula and pulls the inferior angle anterolaterally. These two muscles act as a force couple, causing upward scapular rotation around the root of the scapular spine. When the humerus is raised above 100°, the scapula begins to rotate around the acromioclavicular joint. At this point, the lower trapezius fibers become more active as the lower serratus anterior fibers drag the inferior scapular angle inferolaterally. The muscles’ force couples act synergistically to shift the glenoid to maintain glenohumeral congruity during the humeral elevation. Disruption of the trapezius and levator scapula allows the inferomedial scapular angle to “float” slightly away from the thoracic cage, causing the acromion to tilt toward the greater tuberosity [1,2]. When there are impingement signs on physical examination, and there are no signs of primary impingement on plain radiographs and MRI, then possible causes of secondary impingement, including scapulathoracic dysfunction due to paralysis of the trapezius muscle innervated by the spinal accessory nerve, levator scapula and rhomboid muscles innervated by the dorsal scapular nerve and serratus anterior muscle innervated by the long thoracic nerve.
The DSN pierces the middle scalene muscle at a mean distance of 3 cm (range, 1.8 to 4.5 cm) from its origin at the cervical spine and is more or less centrally located at this exit site. It has a mean distance of 2.5 cm (range, 1.2 to 3.8 cm) medial to the SAN as it travels on the anterior border of the trapezius muscle. The DSN commonly originates solely from the C-5 spinal nerve and rarely from the C-5 and C-6 spinal nerves [3]. The diagnoses of injuries to these nerves are often delayed because the clinical presentation may mimic shoulder impingement or adhesive capsulitis [4].
The SAN is composed of fibers from the anterior horn cells of the upper five and six vertebrae. This nerve may take one or more branches from the cervical plexus or may not take any [5-7].
The levator scapula muscle is often surgically transferred to treat scapular winging caused by trapezius muscle paralysis [8]. Any pathology can affect both muscles because their nerves are in close proximity. Injuries to the SAN are rare, and injury to both the SAN and the DSN is commonly misdiagnosed. Levator scapula and rhomboid muscle transfers are generally indicated for trapezius paralysis with winging scapula, and for this reason alone, these muscles should be examined for DSN injury. The presented case illustrates that DSN function should be kept in mind and be evaluated with posterior SAN palsy resulting from cervical triangle traumas. A patient with SAN palsy may shrug the effected shoulder if the levator scapulae muscle is not affected. In contrast, a patient with both SAN and DSN palsies would be unable to shrug the effected shoulder [9]. Trapezius palsy alone is usually compensated by straining of rhomboids and levator scapulae. This compensation cannot be done during both nerve palsies. Physiotherapy should be tailored according the muscle groups that are involved. A sound physiotherapy cannot be done without a complete understanding of the underlying pathology
Saeed et al., reported that rhomboid muscle weakness is best demonstrated by having the patient lower his or her arms from the forward elevated position [10]. When these muscles are paralyzed, the examiner can easily place several fingers under the vertebral border of the scapula. Patients may also report shoulder or neck pain. Some researchers have stated that a DSN injury may produce an unsuspected, and thus an under diagnosed, component of shoulder pain [3]. Furthermore physicians should follow up the winging and understand the time needed for surgical exploration. A simple overlook as to the cause can lead to confusion of healing process.
CONCLUSION
Injuries of the nerves innervating the scapulothoracic muscles may present as impingement of the shoulder joint due to limitation in scapular movements, which must be considered in the differential diagnosis of impingement syndrome. The DSN and SAN are in close proximity at the posterior cervical triangle, and in the presence of SAN palsy, an accompanying DSN injury should be ruled out due to the close proximity of the two nerves.









































































































































{kind=link}