Silent Cerebral Microembolism during Coronary Artery Bypass Graft Surgery
- 1. Department of Neurology, Boston University School of Medicine, Boston, MA, USA
- 2. Veteran’s Affairs, Boston Healthcare System, Boston, MA, USA
Citation
Zuzuárregui JRP, Rayhill ML, Pochay VE, Treanor PR, Babikian VL (2013) Silent Cerebral Microembolism during Coronary Artery Bypass Graft Surgery. J Neurol Transl Neurosci 1(3): 1019.
CLINICAL IMAGE
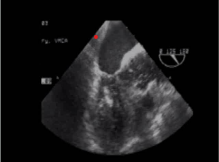
A 62 year-old man with known coronary artery disease underwent a three-vessel CABG after a positive exercise tolerance test revealed reversible ischemic changes. Transcranial Doppler ultrasonography (TCD) and transesophageal monitoring (TEE) were used intraoperatively for monitoring of high-intensity transient signals (HITS), representing both gaseous and particulate cerebral emboli. Non-pulsatile flow was initially seen in the proximal middle cerebral arteries on TCD while the patient was on bypass (Video). Although the single aortic cross clamp technique was used to reduce aortic arch manipulation and release of solid microemboli from the aortic wall, release of the clamp allowed introduction of multiple gaseous microbubbles into the left ventricle and aorta as seen by TEE (Figure 1, Video).

Figure 1 TEE demonstrating left ventricular and aortic root microbubbles (arrows).
Video 1 Gaseous microbubbles entering the left ventricle and aortic root during bypass are seen with TEE monitoring. TCD initially shows non-pulsatile flow, with subsequent cerebral microembolism in both middle cerebral arteries after release of the aortic clamp.
This shower of microbubbles was then detected in the proximal middle cerebral arteries as HITS by TCD monitoring (Figure 2, Video).
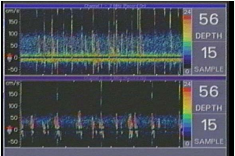
Figure 2 TCD demonstrating cerebral microemboli in the left (top) and right (bottom) middle cerebral arteries.
Post-operatively, the patient did not demonstrate a detectable neurologic deficit.
DISCUSSION
It has been shown previously that cerebral microembolism during cardiopulmonary bypass may negatively impact cognition in the post-operative period [1-3]. For this reason, intraoperative monitoring of HITS by TCD has been used to define the amount of cerebral microembolism that occurs during CABG [1,3]. TCD monitoring is able to detect both air and particulate microemboli as they enter the intracranial circulation, and TEE has emerged in the past decade as a tool to assess the intra-cardiac microembolic load during surgical and peri-operative procedures [4]. Although an overall reduction of cerebral microemboli with the use of proximal aortic anastomosis and membrane oxygenators has occurred, further improvements in peri-operative technique can be achieved with the use of TEE and TCD [1,2,5,6]. For example, intraoperative TCD monitoring of perfusionist interventions during the course of CABG can provide feedback information regarding microembolic load and lead to real-time adjustment to reduce gaseous microemboli introduced into the heart chambers [1,6]. It may also lead to further logistical improvement in the use of bypass, such as changing the position of aortic cannula placement in order to reduce cerebral microemboli [7]. However, large studies have yet to be completed to show whether such intervention can improve clinical outcomes.
TEE and TCD monitoring allow the detection of silent cerebral microembolism during CABG. This case illustrates how monitoring can clarify the impact of intraoperative technique on the microembolic process.
DISCLOSURES
The authors of this study have no disclosures and attest that they have full control of the design of the study, creation of images and videos, and production of the written report.







































































































































{kind=link}