Stuttering Lacunes: An Acute Role for Clopidogrel?
- 1. Department of Neurology, The Johns Hopkins, University School of Medicine, Baltimore, MD, USA
Abstract
Introduction: Intravenous tissue plasminogen activator (IV tPA) has revolutionized the treatment of acute ischemic stroke. However, there remain situations when administration is relatively contraindicated (eg. , arrival outside the accepted treatment window, mild or rapidly improving symptoms). Optimal treatment in these situations is less clear.
Case Series: We describe a small case series of 7 patients presenting with fluctuating symptoms concerning for a capsular warning syndrome (acute isolated motor and/or sensory deficits without cortical signs, usually attributed to small vessel pathology), often referred to as a “stuttering lacune”, who were orally loaded with 300mg of clopidogrel. Four of the 7 patients had complete resolution of their symptoms following the load. The others experienced stabilization of their deficits, but were discharged with mild persistent symptoms. Four patients had evidence of diffusion bright lesions on MRI, while the others had no evidence of infarction. None of the patients experienced hemorrhagic conversion of their infarct or other bleeding complications.
Conclusion: Our experience suggests that acutely loading with clopidogrel may be both effective and well tolerated in the treatment of stuttering lacunes.
Citation
Marsh EB, Llinas RH (2014) Stuttering Lacunes: An Acute Role for Clopidogrel? J Neurol Transl Neurosci 2(1): 1035.
INTRODUCTION
Intravenous tissue plasminogen activator (IV tPA) has revolutionized the treatment of acute ischemic stroke. However, there remain situations (eg., a patient presents outside the accepted time window or experiences rapid improvement of neurologic deficits), when administration is relatively contraindicated. Optimal treatment for these patients is less clear. The Fast Assessment of Stroke and TIA to prevent Early Recurrence (FASTER) trial suggests that administration of dual antiplatelet therapy acutely may reduce early recurrence in patients presenting with minor stroke or transient ischemic attack (TIA), [1] but was significantly underpowered.
We describe a small case series of patients presenting with fluctuating symptoms concerning for a capsular warning syndrome (acute isolated motor and/or sensory deficits without cortical signs, usually attributed to small vessel pathology) [2], often referred to as a “stuttering lacune”, who were orally loaded with 300mg of clopidogrel.
CASE PRESENTATION
A 53 year-old woman with history of hypertension was transferred from an outside hospital with a waxing and waning ataxic hemiparesis. At noon, she noted that her right hand seemed “clumsy. ” She was unable to pick up the phone and her coffee mug “felt funny” when she tried to lift it. At 4PM, her right leg became heavy, as if it was going to give out from under her. Over the course of the evening these symptoms waxed and waned. The following morning when she noted continued difficulty climbing the stairs she made an appointment with her primary care physician. Her systolic blood pressure was over 200mmHg. She was sent to the Emergency Department (ED). In the ED, her blood pressure was 228/130 and it was noted that symptoms worsened with aggressive lowering of her systolic blood pressure to the 130s with intravenous labetalol. An MRI of the brain was performed that showed a diffusion bright lesion in the left internal capsule with corresponding hypointensity on ADC consistent with an acute ischemic stroke (Figure 1A).
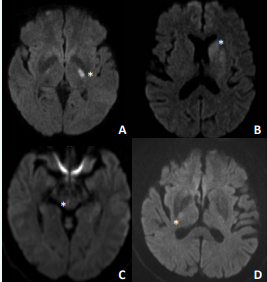
Figure 1 Diffusion weighted MRIs of Patients 1,3,4, and 7 showing diffusion bright lesions in: A) internal capsule, B) corona radiata, C) midbrain, and D) internal capsule consistent with small vessel acute ischemic strokes. An * marks the site of diffusion restriction for each case.
She was transferred to Johns Hopkins Bayview for further evaluation and management. On admission, her NIH Stroke Scale was 7 for mild dysarthria and hemiparesis (strength 4 of 5) with ataxia; however, symptoms dramatically waxed and waned throughout her hospitalization. At lower blood pressures, she developed significant dysarthria, a prominent facial droop, and dense hemiparesis (2 of 5 strength; unable to lift her arm or leg against gravity). A CT angiogram of the head and neck revealed no large vessel stenosis. An echocardiogram showed no evidence of a cardioembolic source. Given her clinical presentation, risk factors, and imaging characteristics, it was determined that her stroke was most consistent with a small vessel lacune secondary to hypertension. Because of her stuttering symptoms, she was loaded with 300mg of clopidogrel based on the FASTER protocol [1]. She had not been on an antiplatelet agent prior to admission. Fluctuations in exam ceased following the clopidogrel load. Treatment resulted in near complete resolution of her deficits, even at lower systolic blood pressures. She was started on 325mg of aspirin and a statin for secondary stroke prevention, and was able to be discharged to a rehabilitation facility with only minor decreased fine motor strength in her right hand.
Six additional patients have presented to our institution with symptoms consistent with a stuttering lacune (average NIHSS 3.7) and been loaded with clopidogrel in the acute setting following a head CT to rule out intracranial hemorrhage. Further details summarizing the characteristics of these patients are summarized in Table 1.
Table 1: Characteristics of patients loaded with clopidogrel.
|
Patient |
Age |
Race |
Gender |
Presenting Symptoms |
NIHSS (worst) |
DWI Abnormality |
Location |
Improvement |
|
*1 |
53 |
White |
Female |
ataxic hemiparesis |
10 |
yes |
internal capsule |
hand weakness |
|
2 |
58 |
Black |
Male |
hemi-body numbness, hemiparesis |
3 |
no |
|
resolved |
|
3 |
57 |
W |
F |
dysarthria, hemiparesis |
8 |
yes |
corona radiata |
arm weakness |
|
4 |
55 |
W |
M |
diplopia, hemiparesis |
3 |
yes |
midbrain |
hemiparesis improved |
|
5 |
52 |
B |
F |
dysarthria, hemiparesis |
3 |
no |
|
resolved |
|
6 |
78 |
W |
M |
clumsy hand, dysarthria |
2 |
CT only |
|
resolved |
|
7 |
64 |
W |
M |
hemiparesis |
3 |
yes |
internal capsule |
resolved |
*Representative Case
Four of the 6 had complete resolution of their symptoms (discharge NIHSS 0) following the load. The other two experienced stabilization of their symptoms and stopped fluctuating, but were discharged with mild persistent deficits (average NIHSS 1). Following the clopidogrel load, all patients were placed on aspirin 325mg. They underwent a basic stroke work-up including: neuroimaging, vascular imaging, echocardiography, and laboratory studies. Three patients had evidence of diffusion bright lesions on MRI (Figure 1) while the others had no evidence of infarction. Following work-up, small vessel pathology was felt to be responsible for the neurologic symptoms of all 7 patients. All patients were treated according to standard of care, including evaluation by physical, occupational, and speech therapy. The typical length of stay was 2-3 days. None of the patients had hemorrhagic conversion of their infarct or other bleeding complications.
DISCUSSION
The capsular warning syndrome is a well described clinical phenomenon [2]. Patients, typically with small vessel risk factors, present with one of the classic lacunar syndromes as described in 1982 by C. Miller Fisher [3]. Symptoms wax and wane in intensity-often ranging from mild to dense hemiparesis in a matter of minutes. Anecdotally, these patients can be misdiagnosed as having recurrent TIAs. This “stuttering” of symptoms can be distressing to both the patient and physician. Before the results of the IST trial, [4] the capsular warning syndrome was occasionally treated with intravenous heparin. Now antiplatelet therapy is used. Despite conventional treatment, the majority of patients go on to irreversible infarction and significant clinical deficits [2-3].
There is some basis in the literature for the acute treatment of vascular events with 300mg of clopidogrel. In 2001, the Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) trial showed that patients with non-ST elevation myocardial infarction had better outcomes at one year after an initial load of 300mg of clopidogrel followed by dual antiplatelet therapy, than those treated with aspirin alone [5]. Subsequently, CLAIR and CARESS showed that acute treatment with dual antiplatelet therapy (including a 300mg clopidogrel load) versus aspirin alone in large vessel cerebrovascular disease resulted in fewer microemboli observed by transcranial doppler, a surrogate marker for recurrent stroke risk [6-7]. Unfortunately, both studies were underpowered to show any difference in clinical outcomes (too few recurrent strokes observed).
The use of dual antiplatelet therapy in general for secondary stroke prevention has been more extensively investigated, with mixed results. Multiple large, randomized, placebo controlled studies (CHARISMA, MATCH, ESPS-2, ESPRIT) suggest that adding clopidogrel or dypyridamole to aspirin may decrease the risk of recurrent ischemia, particularly in certain groups of patients; however, the benefit was typically outweighed by the increased risk intracranial hemorrhage or other severe bleeding [8-11]. Recently, publication of the results from SPS-3 confirmed that, even with minor strokes, the rate of increased bleeding over a mean follow-up of 3.4 years was far greater than the reduction of recurrent ischemic events [12]. None of these studies examined loading with clopidogrel or the role of dual antiplatelet therapy in the acute setting. However, patients with intracranial stenosis enrolled in the SAMMPRIS trial who were treated with dual antiplatelet agents along with high dose statin therapy in the acute setting had lower rates of stroke recurrence in the first 90 days than previously published studies [13]. Additionally, the FASTER trial attempted to show that acute treatment with dual antiplatelet therapy may improve outcomes for other stroke subtypes by enrolling all patients with “minor strokes” (NIH Stroke Scale scores of <4). Unfortunately, the study was stopped prematurely secondary to issues with recruitment [1].
POINT is a randomized, double-blinded trial designed to investigate whether dual antiplatelet therapy acutely in patients presenting with minor strokes (NIHSS <4) and TIAs results in better outcomes. Recruitment is currently ongoing. Until the data has been published, we must continue to rely on smaller case series such as ours to determine the best course of treatment in individuals with minor strokes, particularly when they present with waxing and waning symptoms and are not good tPA candidates. Our experience suggests that acutely loading with clopidogrel is effective and well tolerated.
It is possible that the patients in our series would have symptomatically improved on their own without treatment. However, the natural history of capsular warning syndromes is to progress to infarction [2-3]. Patients presenting with small deep lacunes do tend to recover well over the long term; however, we would argue that they commonly require short term physical therapy. The majority of our patients who were loaded with clopidogrel left the hospital completely, or nearly symptom free.
The risk of bleeding secondary to loading with clopidogrel is unclear. In general, small strokes are believed to have a lower risk of hemorrhagic conversion [14]. None of the patients that we have treated to date experienced intracranial hemorrhage. Additionally, by loading acutely with clopidogrel and then treating with aspirin alone rather than continuing dual antiplatelet therapy, we derive the benefit of the initial load without assuming the increased bleeding risk over the long term seen in previous studies.
Our case series is not without limitations. It is based on only a small number of patients who were not randomized. The average age was also only 59.6 years. Though hypertension, hyperlidemia, drug use, smoking, and other vascular risk factors are prevalent in our population, and lacunar strokes in this age group are not uncommon, the younger age of our patients may result in poor generalizability, and raises the question of whether higher rates of hemorrhagic conversion may be seen in older individuals [14].
In conclusion, for stuttering small vessel lacunar syndromes in patients who do not meet criteria for treatment with IV tPA, there may be a role for orally loading with clopidogrel. In our small case series it appeared to be both effective and well tolerated. We await the results of POINT to elucidate the issue further.









































































































































{kind=link}