The Vanishing Clot
- 1. Department of Neurology, Johns Hopkins University, Baltimore MD, USA
Citation
Marsh EB, Ng K, Llinas RH (2013) The Vanishing Clot. J Neurol Transl Neurosci 1: 1006
CLINICAL IMAGE
A 57 year-old woman with a history of a pulmonary embolus and deep vein thrombosis, on warfarin, presented with the acute onset of right hemiparesis, aphasia, and altered mental status. Her NIH Stroke Scale was 20. Her INR was found to be subtherapeutic at 1.5. The initial non-contrast head CT showed extensive clot in the M1 segment of the left middle cerebral artery (MCA) (arrow, Figure 1A).
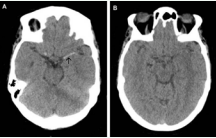
Figure 1A. Non-contrast head CT shows extensive clot in the M1 segment of the left middle cerebral artery (arrow). B. Complete resolution 30 minutes after treatment with intravenous tPA
Intravenous tissue plasminogen activator (IV tPA) was administered 2 hours after the onset of symptoms. Thirty minutes into the infusion, the patient developed a 6/10 headache. On repeat examination, NIH Stroke Scale was now 0. A head CT showed complete resolution of the clot (Figure B).
IV tPA improves longterm outcomes for patients presenting with acute ischemic stroke within 4.5 hours of symptom onset who meet NINDS criteria [1,2]. Unfortunately, recanalization, particularly of large vessel occlusions, is not seen in all patients [3]. There has been recent debate as to whether individuals with occlusions involving the distal internal carotid artery, MCA, and anterior cerebral artery (T lesions), may be best served by “chasing” IV tPA with intra-arterial (IA) therapy [4] or proceeding directly to IA intervention without attempting IV lysis [5]. This case illustrates that IV tPA can be effective in the presence of a hyperdense MCA sign, and should be administered without delay. “Time is brain”.









































































































































{kind=link}