Virtual Reality Arm Supported Training Reduces Motor Impairment In Two Patients with Severe Hemiparesis
- 1. Department of Kinesiology, Pennsylvania State University, 29 Recreation Building, University Park, PA 16802, USA
- 2. Department of Neurology, Penn State Hershey Medical Center, 500 University Drive, Hershey, PA 17033, USA
CITATION
Przybyla, Good DC, Sainburg RL (2013) Virtual Reality Arm Supported Training Reduces Motor Impairment In Two Patients with Severe Hemiparesis. J Neurol Transl Neurosci 1(2): 1018
INTRODUCTION
Stroke is one of the leading causes of motor disability in the United States [1]. Although conventional therapies involve different forms of movement practice, technological advances have allowed the development of interactive therapies using robotics and other computer based interventions, such as virtual reality and computer games. These approaches have the advantages of monitoring movement features on a continuous and incremental basis, as well as providing feedback to patients about instantaneous performance. To date, such approaches have overwhelmingly focused on patients with mild motor deficits [2]. This is likely related to the fact that motor disabilities reduce a patient’s ability to interact with such systems, and because patients with more severe disorders show smaller responses to intervention. In fact, a recent review by Coupar and colleagues suggested that the level of initial severity of motor deficits is the most important predictive factor for recovery of function in the upper limb [3]. Patients with moderate to severe paresis tend to have limited active range of motion due to decreased voluntary control, abnormal synergies, and spasticity. However, movement range can be systematically increased when the limb is supported against gravity in patients with moderate to severe paresis [4-6]. We now combine the approaches of supporting the arm against gravity with a virtual reality interactive design that is tailored to the patients’ abilities in two individuals with chronic and severe hemiparesis. The patients’ arms are supported on a friction free air-sled system to remove the effects of gravity and friction and optimize range of motion in the horizontal plane. We present an interactive computer-game system using our custom virtual reality display system, adjusting the gain of the feedback to encourage maximal engagement in the game-like reaching task. We then adjust feedback gains, in accord with improvements in movement amplitude, in order to encourage continuous adaptation. We evaluate a 4-week training regime by assessing reaching performance during a 3-dimensional unsupported reaching task, as well as, assessing changes in dysfunction level, using the Fugl-Meyer Motor Assessment (FMA) protocol [7]. Following a 4-week training protocol, involving 3 one-hour sessions per week, our results show significant improvements in movement range and quality during unsupported reaching and clinically significant improvements in the FMA of sensorimotor dysfunction.
METHODS
Patients: Two unilateral right hemisphere damaged (RHD) chronic stroke patients gave informed consent in accordance with the Declaration of Helsinki (1964) to participate in this study approved by the Institutional Review Board of the Penn State Milton S. Hershey Medical Center. Both patients had no history nor presence of (i) substance abuse or other significant psychiatric diagnosis (e. g. , psychosis) ; (ii) non-stroke neurological diagnoses; or (iii) peripheral movement restrictions, such as neuropathy or orthopedic disorders. Prior to therapy, patient 1 scored 19, while patient 2 scored 9 points on the upper-limb portion of the FMA, indicating severe impairment in both patients. Patient 1 was 28 months and patient 2 was 44 months after their first and the only stroke occurrence.
System: Our training paradigm was implemented using a virtual reality motion tracking system, Kinereach®, designed by one of the authors (RLS). This system records 3-Dimensional 10 degree of freedom (DOF) motion of each arm at 130 Hz using Flock of birds motion sensors (Ascension Technology, USA). The arm is supported on an air cushion sled that uses continuous pressurized airflow to support the limb against gravity and reduce friction. The result is that the arm is free to move in the horizontal plane, without effects from friction with the table top, nor the need to support the arm against gravity using shoulder abductor musculature.
As shown in figure 1,
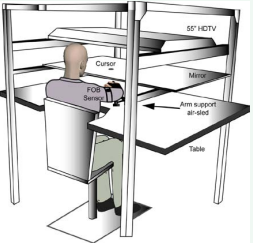
Figure 1 Experimental setup.
the tasks were reflected from TV screen onto mirror, which occludes view of the arms during movement. The distance of the mirror from the arm is adjusted to provide the illusion that the projected stimuli are in the plane of the hand. We provide feedback of hand position as a cursor (much like a computer mouse). While this cursor can be veridical, relative to the position of the hand (Index MCP), this feedback can also be distorted to provide the illusion of greater and more accurate movement displacement. This allowed virtual feedback about movements that could encourage participation, even when movement range was extremely limited.
Task: We presented a start position and 8 targets (center-out design) of equal angular range around the central target. The start position was provided at position in which the arm could comfortably achieve in the horizontal plane. The targets were arranged at a distance 15 centimeters radially from this start position. A single target and start position was shown on the screen. When the subjects’ arm rested within the start position for 1 second, an audiovisual ‘go’ tone was given and the subject was to move the cursor to the displayed target. The subject was given 5 seconds to bring the hand within the target, and was awarded points for accuracy.
Sessions: Subjects performed 3 one hour sessions per week, on a monday-wed-friday schedule, resulting in 12 complete sessions per protocol. Prior to the first, and following the last session, the patients were subjected to a 3-D unsupported reaching test, and the FMA to determine the extent of generalization to a more natural movement environment, and the effect of training on level of dysfunction.
Feedback Gains: Each training session consisted of two blocks of practice, with 15 minutes break in between blocks. Each block consisted of 176 trials, 22 cycles to 8 targets. The first two cycles (16 trials) were used to calibrate the visual feedback gains to each target, as follows: Visual feedback gains were adjusted to compensate for each patient’s errors in axes parallel and perpendicular to the target direction: Increases in gain parallel to the target direction increased the amplitude of cursor motion toward the target, relative to hand motion. Decreases in gain perpendicular to the target direction decreased direction errors relative to the target. We adjusted these gains for each target direction in order to produce fairly isotropic cursor displacements across movement directions. This required substantial modifications in gain, as motion away from the body was severely restricted (note figure 2)

Figure 2 Exemplar hand-paths of movement performance of severe stroke patient 1 (FMA=19) in the unsupported (left panel) and the air-sled supported (right panel) reaching to targets revealing extensive movement deficits.
in the initial session. For example, if the patient was able to move only half distance to a given target, the parallel visual gain was doubled, so that the cursor reached the target on the screen despite patient’s deficits.
During the course of training, these gains were interactively reduced, as patients increased the range and accuracy of their movements. Gains changes were done on a 5% change, when the prior movements increased amplitude or directional accuracy by 5%.
Dependent Measures: We evaluated the effects of the intervention by quantifying measures of movement quality during both supported and unsupported (3-D) reaching: Cumulative movement distance (Dist), Shoulder and Elbow joint displacement (JD), peak velocity (Vmax), movement Time (MT), Error in movement direction (DE) and accuracy (FPE) at movement completion Motor performance to targets that yield the most extensive motor deficits in unsupported reaching prior to therapy were subjected to nonparametric statistical comparisons with the alpha value set at 0.05. We found that in both patients, the most impaired movements were those that required elbow extension, thus for the purpose of statistical analysis we collapsed trials across three targets away from the start position with respect to the body.
RESULTS
Figure 2 shows hand-paths of patient 1 (FMA=19) prior to intervention (in gray) and following the four week intervention program (in black) for unsupported (left) and supported (right) reaching movements, using the paretic arm. Prior to training, movements toward these targets were incompletely executed, due to limited active range of motion. The movements toward the leftward target (135°) initially showed the most limited range. In Figure 3,
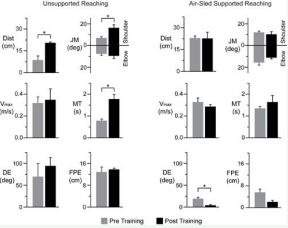
Figure 3 Averaged movement performance of stroke patient 1 (FMA=19) in the unsupported (left panel) and the air-sled supported (right panel) reaching.
we summarize averaged motor performance before (gray) and after (black) training for both unsupported (left) and supported (right) reaching. Initially, unsupported reaches toward these targets moved only an average of 1/3 of the distance (0.07±0.03 m). Note that supported movements (right) showed greater distance, but in the wrong direction (see figure 2), with on average 50±14 deg direction error. Thus, the support allowed greater range, but not greater coordination. As can be seen, the increased motion in the supported movements was due to increased shoulder, but not elbows motion. As seen from the plots (asterisks indicate significance), unsupported movements were initially (gray) slow, with large direction and final position errors. However, following training under air-sled supported conditions, the quality of movements with support (right panel) showed trends toward improved distance, elbow excursion, speed, and distance, but these improvements were not statistically significant. Nevertheless, transfer of movement practice to 3-dimensional unsupported movement conditions was significant. Subjects showed an almost tripling of movement distance, associated with increased speed, and substantially decreased direction and final position errors. These improvements were associated with an increase in elbow and shoulder excursions that did not reach significance.
Thus, practice under supported, gain modified, conditions ed to substantial improvements in unsupported natural reaching conditions. In addition, this patient showed a 5 point improvement in FMA score, at the end of intervention, confirming generalization of intervention to natural sensorimotor conditions. In fact, improvements in FMA scores from 4.25-7.25 are considered clinically significant [8]. These findings suggest that this treatment approach might lead to substantial improvements in motor function for patients with severe hemiparesis.
We next examine a patient with more profound deficits, with a pre-treatment FMA score of only 9. Figure 3 shows averaged motor performance from this patient prior to (gray), and following (black) the 4 week intervention program. Generalization to natural unsupported reaching is reflected by significant improvements in movement distance, which is associated with significantly increased shoulder joint excursion and movement time. However, these improvements were not associated with other measurements of movement quality during unsupported reaching. During supported reaching, slight and significant improvements in movement quality were revealed by a significant increase in directional accuracy. Interestingly, this patient also showed an improved FMA score from 9 to 14. In summary, our intervention showed promising improvements in movement quality that transferred to the untrained natural condition of 3-D unsupported reaching and to the clinical FMA score. However, these effects were substantially greater in the patient with the less profound motor deficit.
CONCLUSIONS
Our preliminary results suggest that chronic stroke patients with severe and even profound hemiparesis are able to make significant improvements to movement range and quality during untrained unsupported reaching movements, as a result of airsled supported reaching training with adjustable visual feedback gains. However, consistent with previous reports [3] our results also suggest that these effects vary with the severity of the initial movement deficits. Both patients showed significant increases in the range of unsupported movements, but this change was only associated with improvements in speed and reductions in errors for the patient with less profound initial motor deficit. Given the duration and intensity of this training, we suggest that these improvements are of substantial clinical value, as suggested by the improvements in clinical assessment. Whereas many studies have suggested that improvements in motor function in patients are extremely limited in chronic stroke patients with severe and profound paresis [2], we believe that our current results provide an encouraging outlook for the use of technological interventions with such patients. This technique builds on the work of Dewald and coworkers, who have demonstrated that chronic stroke patients with severe hemiparesis can benefit from movement practice under conditions in which their arms are supported against gravity [4-6]. In those studies, patients were provided graded decreases in gravitational support during the course of training, which transferred to significant improvements in unsupported reaching. In the current study, we combine this approach with graded changes in visual feedback that encouraged increases in movement distance during the course of training. Further studies using this technique are necessary to identify mechanism of such improvement in patients with severe and profound movement deficits. This was the first step towards development of novel therapy for moderate to severe stroke patients and our currently presented design did not differentiate between the air-sled arm support factor and visual feedback gain adjustments. However, our results are very promising and we believe that further studies to identify mechanism of such improvement in severe stroke patients would be very valuable for clinical rehabilitation community.
ACKNOWLEDGMENTS
This research was supported by the National Institute of Health grants R01HD39311 and 30 R01HD059783 to R. L. Sainburg.







































































































































{kind=link}