Heavy Drinking and Treatment among HIV or HCV Co-Infected Patients
- 1. New York State Psychiatric Institute, USA
- 2. Department of Psychiatry, Columbia University Medical Center, USA
- 3. Division of Infectious Diseases, Columbia University Medical Center, USA
- 4. Department of Epidemiology, Mailman School of Public Health, Columbia University, USA
ABSTRACT
Aims: Given the efficacy of new medications for Hepatitis C virus (HCV), we aimed to determine whether drinking relates to HCV treatment access among the high-risk group of individuals with HIV/HCV co-infection.
Methods: We sampled 210 patients in a sexual health clinic; of these, 39 reported HIV/HCV co-infection (79.49% male; 56.41% Black). Patients completed a self-report survey on drinking and treatment history.
Results: Those drinking despite health problems reported less HCV treatment (p=0.035). Drinking despite health problems did not relate to whether HCV treatment was recommended by providers, and binge drinking did not relate to either HCV outcome. Drinking was unrelated to HIV treatment.
Conclusions: HIV/HCV co-infected individuals drinking despite health problems are in urgent need of attention, to reduce drinking and increase engagement in treatment. Drinking despite health problems may serve as an effective screening question to identify HIV/HCV co-infected drinkers who are most at risk of being untreated.
KEYWORDS
• HIV
• Hepatitis C
• Alcohol
• Drinking
• Treatment
CITATION
Elliott JC, Shalev N, Hasin DS (2018) Heavy Drinking and Treatment among HIV/HCV Co-Infected Patients. J Subst Abuse Alcohol 6(2): 1079.
ABBREVIATIONS
HIV: Human Immunodeficiency Virus; HCV: Hepatitis C Virus
INTRODUCTION
Individuals co-infected with HIV and Hepatitis C virus (HCV) constitute a high-risk population for whom heavy drinking is particularly dangerous. These individuals face increased health risks when compared with those with HIV or HCV alone [1]. Although HCV alone can cause liver damage, HIV accelerates this progression [2]. Direct-acting antiviral (DAA) medications to treat HCV demonstrate increased efficacy and tolerability over prior regimens, in both HCV and HIV/HCV co-infected patients [3]. However, patient alcohol consumption can impede successful HCV outcomes.
Heavy drinking can accelerate liver damage (notably in co-infected patients) [4], and increases the risk for fibrosis [5] and hepatocellular carcinoma [6] even after sustained virologic response for HCV has been obtained. The combined risks of HCV, HIV, and heavy drinking have been termed a “perfect storm” in this “understudied and underserved” population [1]. Yet, although one study suggested that HCV co-infection is associated with less drinking in the HIV population [7], other research suggests that HCV co-infection is associated with more drinking [8], potentially interfering with successful treatment.
Hepatitis C guidelines by the American Association for the Study of Liver Diseases and the Infectious Diseases Society of America state that “Abstinence from alcohol and, when appropriate, interventions to facilitate cessation of alcohol consumption should be advised for all persons with HCV infection” [9]. Although this is consistent with alcohol’s potential harms, these similar guidelines may limit access to treatment when they are enforced by requiring alcohol abstinence or treatment for problem drinking as prerequisites to reimbursement for HCV treatment [10]. Despite efforts to increase accessibility of HCV medication for all, emerging research suggests that heavy drinkers with HCV and HIV/HCV sometimes have difficulty accessing DAA medication [11]. More research is needed on this topic, particularly among HIV/HCV co-infected patients. Identification of a brief screening question to identify those most at risk for problematic drinking and lack of treatment would be particularly useful. Toward this goal, we examined whether HIV/HCV co-infected individuals who drink heavily are less likely to be recommended and to receive HCV treatment. We also conducted parallel analyses on HIV medication access in these same individuals.
MATERIALS AND METHODS
Participants and procedures
Patients consecutively presenting for treatment at an urban sexual health clinic were approached in the waiting room and invited to complete a brief anonymous survey on a tablet (Elliott et al., under review). Surveys were conducted in a separate room to ensure privacy. Patients read a consent statement and clicked forward to indicate consent, in compliance with the approved protocol by New York State Psychiatric Institute’s Institutional Review Board. A total of 210 patients completed the survey, and received a round-trip subway fare card (value: $5.50) as compensation for their participation. Patients were asked whether they were infected with HIV, and whether they had ever been told that they had HCV. Current analyses use the subset of patients who responded affirmatively to both HIV and lifetime HCV (n=39).
The subsample of HIV/HCV co-infected patients were on average in middle adulthood (mean age = 53.08 [SD = 11.31]), mostly male (79.49%; 17.95% female; 2.56% transgender), mostly racial/ethnic minority (56.41% Black; 25.64% Hispanic; 15.38% White; 10.26% Native American; 7.69% other; multiple endorsements allowed), and most had completed high school or a GED (84.62%).
Measures
Patients reported on the number of days in the past month in which they had four or more drinks, dichotomized to indicate the presence or absence of any past-month binge drinking. They were also asked whether, in the past month, they had ever continued to drink even though it was causing a health problem or making a health problem worse. This question was chosen to measure drinking despite known harm, a concerning behavior for individuals with serious medical problems, and a symptom of alcohol use disorder.
Regarding HCV treatment, participants were asked whether their medical provider had ever recommended HCV medication, and whether they had ever taken HCV medication. Regarding HIV treatment, participants were asked whether their medical provider had ever recommended HIV medication, whether they were currently taking HIV medication, and if not, if they had ever taken it.
Analysis plan
We assessed the associations of both dichotomous drinking variables (binge drinking; drinking despite health problems) with HCV treatment (ever recommended HCV medication; ever taken HCV medication) and with HIV treatment (currently on HIV medication; ever taken HIV medication). All had been recommended HIV medication, prohibiting analysis of this variable. Data were analyzed using Chi-square tests, or Fisher’s Exact Tests for smaller cell sizes; significance was indicated by p<0.05.
RESULTS
Regarding HCV treatment, drinking despite health problems was associated with a lesser likelihood of ever engaging in HCV treatment (Fisher’s Test, p=0.035; Figure 1).
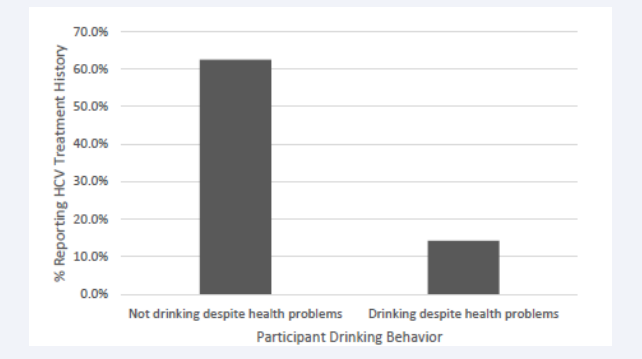
Figure 1: Hepatitis C Virus (HCV) treatment status by drinking despite health problems among HIV/HCV co-infected individuals.
Of those who drank despite health problems, only one in seven had ever had treatment. Of those who did not drink despite health problems, almost two thirds (20 of 32; 62.5%) had received treatment. Drinking despite health problems did not relate to whether HCV treatment had ever been recommended (Fisher’s Test, p=0.99), and binge drinking did not relate to either HCV outcome (recommended: Fisher’s Test, p=0.99; treated: X2 (1) =1.88, p=0.17).
Neither drinking variable was associated with current or lifetime HIV treatment. Specifically, binge drinking was unrelated to current (Fisher’s Test, p=0.55) and lifetime (Fisher’s Test, p=p=0.99) HIV treatment, as was drinking despite health problems (current: Fisher’s Test, p=0.46; lifetime: Fisher’s Test, p=0.99).
DISCUSSION AND CONCLUSIONS
In this sample of HIV/HCV co-infected individuals, those who drank despite health problems were less likely to have had HCV treatment than those who did not drink despite health problems.
This suggests that risk behaviors such as drinking despite known risk and not engaging in HCV treatment may cluster together, with potential damaging effects. There was no difference in whether patients drinking despite health problems reported that their providers recommended treatment, suggesting that this was not due to unwilling providers. Yet, the low numbers of co-infected problem drinkers utilizing HCV treatment is concerning, as these individuals are arguably most in need of liver-related treatment. Further research should aim to better understand how problem drinking and lack of engagement in HCV treatment relate, and what can be done to better engage these individuals in HCV and alcohol treatment. Our study demonstrates the potential value of asking about the alcohol use disorder symptom of drinking despite health problems in particular, which may help identify individuals at high risk of being out of treatment. There were no significant associations between drinking and HIV treatment, suggesting that this phenomenon was specific to HCV treatment, although the vast majority of patients were on HIV treatment.
The current study highlights the lack of HCV treatment in a high-risk group: HIV/HCV co-infected patients who drink despite health problems. Although our sample was small (necessitating use of Fisher’s Exact Tests in most analyses) and methods relied on self-report, certain clinical indicators (e.g., HCV co-infection rate) mirrored known characteristics of the clinic population at large. Low levels of treatment engagement among co-infected individuals who drink despite health problems highlights a need to improve HCV treatment access in this high-risk group. Use of drinking despite health problems as a screening question may facilitate future research in this area. Further research and treatment should seek to improve treatment engagement among HIV/HCV co-infected problem drinkers.
ACKNOWLEDGEMENTS AND FUNDING
We thank Sofia Dubitsky, MS, for her assistance in data collection, and the staff at the sexual health clinic for their participation. This work was supported by the National Institutes of Health [grants K23AA023753 (to JCE), R01AA023163 (to DSH)]; and by the New York State Psychiatric Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.










































































































































{kind=link}