Using an Epidemiologic Lens to Develop a National Comprehensive Substance Use Service Delivery System
- 1. President, Applied Prevention Science International, USA
- 2. Senior Scientist, University of North Carolina-Chapel Hill, USA
Abstract
The intersection of epidemiology and medical science forms the basis of a public health approach to challenging health issues. Although initial conceptions of epidemiology predominantly focused on infectious diseases, the epidemiological approach has been applied successfully to non-infectious or non-communicable diseases including those health issues related to substance use. However, unlike an infectious disease or even a chronic condition such as cancer, substance use is more dynamic with changing forms of the external agent—psychoactive substances-- and the variety of sources for these ‘agents’ that may vary geographically (within and across communities), as well as sociologically (involving a variety of social groups across time and space). As such, the dynamic nature of substance use warrants an epidemiologically-informed system for its prevention and treatment, that includes Ongoing monitoring and dynamic and timely surveillance systems designed to identify emerging patterns of use with implications for prevention and treatment, such as new ways to administer substances (e.g., injecting crack cocaine), new ‘mixtures’ of substances (e.g., changing the composition of substances such as mixing fentanyl with heroin or Adderall), new types of substances, and new user groups. This paper demonstrates how this type of epidemiologic information can inform the structure and function of a national comprehensive substance use service delivery system to address the issue on a population level.
Keywords
• Epidemiology
• Substance Use
• Comprehensive
• Service Delivery System
Citation
Sloboda Z, Fishbein DH (2026) Using an Epidemiologic Lens to Develop a National Comprehensive Substance Use Service Delivery System. J Subst Abuse Alcohol 13(1): 1108.
WHAT DO WE KNOW ABOUT THE EPIDEMIOLOGY OF SUBSTANCE USE?
In the past, use of alcohol, tobacco and other ‘legal drugs’, and ‘hard’ or ‘illegal/illicit drugs’ were handled differently, largely because the focus of national policies was on treatment rather than prevention [1-4]. Clearly, research on the short-and long-term impacts of all of these substances on the developing brain has now shifted the focus, particularly for prevention efforts, to all substances that affect feelings, perceptions, thought processes, and/ or behavior (UNODC, 2003)—psychoactive substances. There have been relatively few studies on the natural history of substance use that begin in childhood and follow individuals across time to examine what factors or experiences influence trajectories beyond the initial phases of substance use [5-8].
Figure 1 presents a graphic that depicts what we know about the natural history of substance use. Such an understanding can guide the development of an epidemiologic system that operates to determine the types of services required to address the diverse needs of people who use substances in our communities.

Figure 1 Natural History of Substance Use and Substance Use Disorder.
This graphic suggests that most individuals initiate substance use in response to perceived need and environmental factors [9]; however, at some point, the pharmacological effects of the psychoactive substance(s) take hold and dependence can develop [10]. We also know that many who initiate use at some point discontinue use on their own [11-13]. Although not well documented, hypothetically there are those who become dependent who can continue use with no health or other problems— we know very little about this group, which often includes patients experiencing pain—but others will develop problems. This group will need treatment to address the pharmacologic effects of the substances they have become dependent on, and to assist in recovering from detrimental influences on their lifestyle and relationships, and to ease their reintegration into their communities [14].
This understanding and the epidemiologic information we have available suggests that there are eight population groups within a defined population at any given time. Those who:
- Do not use substances and are not ‘vulnerable’
- Do not use substances AND ARE vulnerable, such as children of substance users and who have experienced maltreatment, individuals living in poverty, and other sources of extreme adversity.
- Initiated use and may or may not experience negative consequences.
Meet a DSM diagnosis for treatment but who:
4. Did not seek treatment
5. Sought treatment but did not receive treatment
6. Received treatment and did not complete treatment
7. Received treatment, completed treatment and are in recovery
8. Received treatment, completed treatment and relapsed
Considering these distinct population groups enables us to translate the natural history of substance use disorder into service needs (Figure 2).

Figure 2 Services within the Context of the Natural History of Substance Use Disorder.
Universal prevention programming primarily reaches youth who have not initiated use and operate to evade such use; however, these programs also impact those who are vulnerable and potentially at risk of initiating substance use. Also, as universal programs, they are often delivered to groups of youth that include those who have initiated use and may or may not be experiencing adverse consequence of their use [4]. Selective prevention programming addresses youth who are vulnerable to use but may not yet have initiated use, such as children of substance users. And, indicated prevention programming is designed to meet the needs of those who have initiated substance use (NRC, 1994) [15], to deter progression to abuse. Once use is initiated and the pharmacological effects begin to adversely impact the person, treatment is needed. Research has shown that not everyone who uses psychoactive substances seeks or receives treatment [16], and, even if they do receive treatment and are in recovery, there is a need for implementation of harm reduction strategies, such as in the case of potential relapse or overdose after a period of abstinence [17].
To reach each of these groups with the objective to prevent initiation, escalation and dependence and provide treatment, there is a clear need for research based, community-oriented policies and organizational infrastructures to broadly and systematically implement services. And given the diverse needs of these individuals, an array or spectrum of services from prevention through to treatment and maintenance or reintegration and harm reduction at various population levels are required. Such a spectrum of services has been proposed by the National Research Council [15]. Ending the fragmentation of community-based prevention and treatment programs and integrating them into one service delivery system will strengthen public health and safety as these services would address both the incidence (new cases) and the prevalence of substance use and substance use disorders.
Available monitoring data and research can help to estimate the size of these groups, thus guiding service needs. For instance, at a national level in the United States, available data might be used in the following ways to improve our understanding of the differential needs of each group:
Group 1: General Population Do Not Use Psychoactive Substances: Data from the 2022 National Survey on Drug Use and Health (NSDUH1) show that approximately 60% of persons aged 12 and older used at least one psychoactive substance listed here in the month prior to survey (SAMHSA). Of course, this Figure 3 assumes these are unduplicated estimates; i.e., that those reporting use are only using one type of substance. And it would mean that 40% of the population, 110 million people, did not use any psychoactive substance.

Figure 3 Estimated Distribution of the Population by Group.
Group 2: General Population Who Are Vulnerable: It is more difficult to find out among those 110 million non-substance users how many would fit our ‘vulnerable’ status [18]. A paper by Lipari and Van Horn et al. [19], estimates that 8.7 million children had at least one parent who had a substance use disorder, those most vulnerable to substance use. Monitoring the Future Survey provides data on the misperceptions of harm or risk regarding substance use that also have been found to be associated with initiating substance use. Thus, for instance, in 2022, 20% of eight graders, 17% of 10th graders and 10% of 12th graders thought that smoking marijuana once or twice a week was risky [20]. That means that 80%-90% did not see any risk associated with smoking marijuana once or twice a week. It should be noted that these perceptions of risk have been decreasing over time perhaps as a result of States legalizing the recreational use of marijuana, suggesting that substance use is not harmful.
Group 3: Those Who Initiated Use May Or May Not Experience Consequences: More information is needed to better understand the circumstances under which individuals in the general population initiate use and may or may not experience consequences. There are data from the NSDUH on estimates of past year initiation of psychoactive substances showing that over 70 million people reported “illicit” substance use; however, information regarding consequences of use have not been assessed.
Group 4: Those Who Meet The DSM Criteria Of A Substance Use Disorder Diagnosis But Did Not Seek Treatment: Data are available from NSDUH regarding what proportion of the general population aged 12 and older meets a DSM diagnosis for substance use and need treatment but did not seek treatment. Data on this population indicate that in 2022, 24% or 13.1 million received treatment.
Group 5: Those Who Meet The DSM Criteria Of A Substance Use Disorder Diagnosis And Sought Treatment Did Not Receive Treatment: It is estimated that there are 236,000 individuals aged 12 and older or 1.2% who needed and sought treatment but ultimately did not receive it (SAMHSA, 2020) [21].
Group 6: Those Who Meet The DSM Criteria Of A Substance Use Disorder Diagnosis And Did Not Complete Treatment: Lappan and colleagues et al. [22], estimate that about 30% of those who initiated treatment do not complete it for a variety of reasons.
Groups 7 & 8: Those Who Meet The DSM Criteria Of A Substance Use Disorder Diagnosis And Received And Completed Treatment And Are Either In Recovery Or Have Relapsed: It is not clear as to the percentage of the 13.1 million who received treatment and actually completed it at the time of the 2022 NSDUH. Applying Lappan et al.’s estimates, indications are that this number may be around 9,170,000.
Building an epidemiologic monitoring and surveillance system at the local, state and national levels would provide data on these eight groups, preferably on a periodic basis to not only monitor trends in use patterns but also to identify new and potentially challenging patterns of use (substance, mode of administration, demographics). Of importance, particularly at the local level, are systems that provide both quantitative as well as qualitative methods for data collection. Often neglected are archival databases such as arrests, overdoses, admissions to treatment and local hospitals, family and drug court data, child protective services and foster care data, mortality data, school data regarding absences or in-school infractions related to substance use [23].
In sum, descriptive epidemiology helps to identify groups within a population and provides data to inform hypotheses regarding the processes and determinants associated with an individual’s movement across the natural history of substance use progression.
Developing a Comprehensive and Integrated Substance Use Service Delivery System Supported and Informed by an Ongoing Epidemiologic Surveillance and Monitoring Research System
The epidemiologic picture for substance use presented above mostly pertains to communities across the United States with some variation regarding the availability of psychoactive substances, especially alcohol and tobacco given their prevalence, and others that are equally as consequential. There is also a clear need for a community based integrated and comprehensive service delivery system, such as presented by the National Academy of Sciences, Engineering, and Medicine [21], that provides and sustains evidence-based prevention and treatment services. Such a mandate requires an infrastructure of well-trained prevention and treatment professionals and a monitoring system to assure that quality services are being delivered and desired short-term outcomes are achieved. Currently, the country is experiencing a ‘fractured’ system of services in which the implementation and sustainment of effective prevention and treatment interventions are not materializing [24-26]. This is the case despite the reality that the individual components of such an ideal system are already in place. They only need to be integrated, reviewed to identify gaps, and supported. The UNODC-WHO (2013; 2018, p.59) outlines a prevention service delivery system revealing important components of such a system. These components can also be integrated into a comprehensive integrated substance use service delivery system.
The Structure for a Comprehensive Integrated Service Delivery System.
As Fishbein and Sloboda et al. [27] recommend regarding the development of a prevention service delivery system, it is important to emphasize that the basic unit of the system is the ‘community’ which can be variously defined by population or government boundaries. An array of prevention and treatment services that map to the needs of that community could then be made available and managed through a central organization or agency. The responsibilities of this unit would be to assure that an evidence-based continuum of services is implemented with quality by certified and licensed professionals [27]. These units would also monitor who received what services and report their outcomes. The monitoring instruments would build on existing ones and be used universally across all communities. These community units would report to a state agency that oversees the operations and based on this information provide feedback and if necessary, technical assistance. In turn, state agencies would report to a national oversight agency.
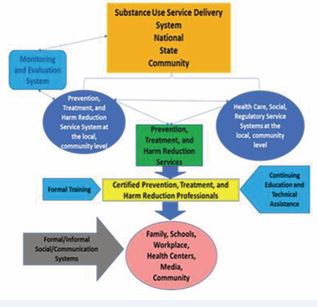
Figure 4 Comprehensive and Integrated Substance Use Service Delivery System.
Figure 4 presents the recommended components of such a system. Although each component part is essential to the functioning of the system, three are key. First is the need to build the integrated service system drawing on the essential evidence-based components and practices associated with prevention, treatment and harm reduction services building on the knowledge base presented earlier. Second is to have a trained, certified and, where appropriate, licensed service delivery staff that share the same knowledge, skills and competencies. Third is having in place a monitoring and evaluation system.
WHAT CURRENTLY EXISTS AND WHAT IS NEEDED TO CREATE THIS SERVICE DELIVERY SYSTEM
Surveillance and Monitoring Systems
Moving to a comprehensive service delivery system warrants a review of existing systems not only for content but also for their relevance to current and emerging patterns of use. Sloboda et al. [28], noted that it may take up to two years before an emergent substance of abuse can be incorporated into existing monitoring systems. This time gap must be addressed to gain a better understanding of the extent to which these emergent patterns exist in the general population. In addition, a warning system is needed to alert substance use or health service providers about these new patterns and what the health consequences are for individuals and whole populations. To date, there is strong evidence that changing demands, expectations, messages, and stresses experienced by children, adolescents, and young adults are not well addressed by existing services [29].
Prevention, Treatment and Harm Reduction Services Research
A great deal of information has been amassed regarding the most effective prevention and treatment services [30 34]. Three major issues remain, however. The first is that there is a need for further research on harm reduction strategies and services. The lack of attention to studying harm reduction approaches is associated with views that harm reduction enables substance use, as well as pervasive stigma against substance users [35]. The AIDS epidemic brought more attention to harm reduction approaches, but barriers, particularly in the use of federal funds for needle exchange programs, limited research to explore these approaches despite strong evidence to support them [36-38]. Harm reduction plays a significant role in the spectrum of services for substance users, from ‘selective’ and ‘indicated’ prevention services through to recovery support and reintegration. To address the spread of diseases such as AIDS, bacterial endocarditis and sexually transmitted infections, it is important to better understand the processes involved in cleaning injecting equipment and using condoms, for example, guiding the development and evaluation of interventions [39,40].
The second is the need to update the research on prevention programs found to be evidence- based with new populations. The culture and life challenges of the current adolescent population are quite different from the populations that participated in the evaluations of the 1980s through the year 2000. A recent review of NIDA funded prevention grants by the Coalition to Advance Prevention Solutions to the Opioid Crisis (CAPSOC- https://www.npscoalition.org/consortium-to-advance prevention-solutions-to-the-opioid-crisis-capsoc) indicated that the majority of funding is supporting HIV related prevention efforts, followed by support of more traditional prevention approaches and ‘normalization’ of proven practices; i.e., integrating prevention strategies into health and social service settings [41-43]. Findings from this research will help guide decisions at the community level as to the most effective preventative approaches for the general population and those more vulnerable to substance use and other risky behaviors. However, there remains a need for more research focusing on the ‘drivers’; e.g., to delineate the mechanisms that both interfere with and boost favorable outcomes. Further research is needed to determine best practices for implementation, with attention to cultural, subgroup, contextual, and other factors that influence adoption, scaling, and sustainment.
U.S.-developed evidence-based prevention interventions are being replicated around the world. Many of these replications are resulting in either no positive outcomes or positive outcomes with lower effect sizes than control or comparison groups, thus diminishing the ‘evidence-based’ designation. More cross-national studies of evidence-based preventive interventions are needed. Of great potential significance is the Adolescent Brain Cognitive Development (ABCD) Study [44], a longitudinal study underway in 21 sites, following 11,000 9-10 year olds over 10 years [45], to understand the role of brain development in substance use using standardized tools and to identify both protective and adverse factors that influence development and subsequent behavior. Also of relevance, in the Healthy Brain and Child Development (HBCD) [46], research initiative, is that the effects of maternal prenatal use of psychoactive substances are under study. However, there is a need for more population-based longitudinal studies of children and adolescents to further examine vulnerability to substance use and other unhealthy behaviors and the influence of the micro- and macro-level environments that protect or place at risk those determined to be vulnerable.
The third research area focusing on treatment presents the same picture as outlined above for prevention; in particular, the need for more implementation research. NIDA has supported the Clinical Trials Network for over 20 years to conduct research: “(1) large multi-site studies; (2) determining how to close the treatment gap; (3) expansion of ongoing studies to improve service delivery and implementation; (4) studies to explore the use of substance use data in electronic health record systems; and (5) training and dissemination projects to expand the research/health care provider workforce” [47]. Of concern is that only about 10%-15% of individuals considered in need of substance use treatment actually receive treatment, as noted in the National Survey on Drug Use and Health Survey [48]. This is a disturbing finding, and yet the research focusing on understanding the hesitancy to access treatment along with developing communication messages that reach and motivate this population has been minimal. Perhaps even more disturbing is the lack of information regarding the availability of treatment services and processes, as well as characterizing providers who are delivering the services [5-50].
Training and Professionalization of Prevention, Treatment and Harm Reduction Service Practitioners
A major challenge is developing the workforce available to provide these services. While the treatment workforce has been well-defined since the late 1970s, prevention and certainly harm reduction have lagged well behind [51-56]. Several groups have contributed to development of guidelines required to understand and implement evidence-based preventive interventions and policies, as well as developmentally appropriate delivery strategies that address the learning needs of the population of focus [27-58]. However, in contrast to treatment, substance use prevention practitioners do not have a U.S. Department of Labor recognition as a professional category and, although the International Credentialing and Reciprocity Coalition (IC&RC) offers a credential for prevention professionals based on experience and test scores, not every state requires this credentialling to provide services. Furthermore, many education, health and social service professionals deliver substance use prevention, treatment, and related harm reduction services yet they do not identify themselves as prevention, treatment or harm reduction professionals. Therefore, there is a need to develop training programs that impart the same knowledge and skill base in the educational and post-graduate trainings of providers who self-identify as prevention, treatment or harm reduction professionals, as well as of those who do not self-identify in these roles but are engaged in delivering these services, such as teachers, law enforcement officers, social workers, public health nurses.
Currently in the U.S., there are at least 7 universities that offer a doctorate in prevention science and 7 that offer a master’s or certificate in prevention science, 6 universities offer a doctorate in treatment and over 30 offer a master’s or certificate in treatment. The Prevention Technology Transfer Centers (https://pttcnetwork.org/) and the Addiction Treatment Technology Transfer Centers (https://attcnetwork.org/) offer webinar and training videos, also. In addition, groups such as the Applied Prevention Science International (www.apsintl.org) offer trainings to active prevention professionals on prevention science and its application to prevention strategies. These trainings should address implementing evidence-based strategies working with parents and families, in schools and the workplace and how to effectively develop policies and prevention-based media messaging. As the focus of the delivery system is the community, trainings should also include developing community infrastructures, such as coalitions, to support comprehensive prevention programming. The National Harm Reduction Coalition also offers trainings in harm reduction strategies (https://harmreduction.org/our-work/training-capacity building/training-center/) and the IC&RC mentioned above (https://internationalcredentialing.org/) provides certificates in for substance use treatment and, recently, for harm reduction.
NEXT STEPS 2
To build an epidemiologically informed comprehensive substance use service delivery system, this paper concludes with the following abbreviated recommendations and plan of action.
Phase I—Problem Assessment and Framing the Elements of a Strategic Plan. A two-day in-person meeting including approximately 25 leaders including substance use epidemiologists, prevention, treatment, and harm reduction researchers and practitioners, law enforcement, judiciary, schools, families, communities, policy makers, and health services. The outcome would be the development of a community/local-based integrated comprehensive substance use service delivery system model that identifies challenges to building such a system. Information gathered in this meeting will then be used to develop the design of an initial framework--a prototype—and a monitoring and evaluation plan to demonstrate efficacy and effectiveness. The plan will be guided by a logic model that includes goals, objectives, performance outcomes, and key actions for successful implementation. The plan will also outline recommendations and implementation steps.
Phase II—Expanded Stakeholder Involvement: The final draft comprehensive strategy will be disseminated to the public and an expanded team to get input and support for a community/local-based integrated and comprehensive service delivery system and for the concept of demonstrations. These additional planners shall represent community stakeholders and will participate in the co-creation of acceptable, appropriate and effective implementation approaches.
Phase III-Define and Build a Model Comprehensive Substance Use Service Delivery System.
Based on the outcomes of Phases I and II, a model comprehensive substance use service delivery system with corresponding guidelines for its construction will be developed and implemented. It is recommended that at least five demonstration sites be established and closely monitored and evaluated. Based on this experience, teams of trainers will be formed to work with communities to build and implement these systems within each state. These trainers will also serve to provide technical assistance as needed. The PTTC and ATTC networks are ideal for the implementation of this phase.
Phase IV—Develop Training and Technical Assistance Protocols to Professionalize the Prevention, Treatment and Harm Reduction Services Workforce.
Working with universities and prevention, treatment, and harm reduction specialists and representatives of IC&RC and professional groups, develop a comprehensive training program drawing from existing programs mentioned above. This phase would train professionals both through a degree program and through Continuing Education. Training would ultimately credential individuals through the International Certification and Reciprocity Consortium based on work experience and test scores with quality upgrades over time. Technical assistance would also be provided to communities to build an implementation system that supports prevention, including health and social services, schools, parent groups, businesses, law enforcement and the judicial system. In addition, such a system will require professionals trained in implementation science who have been trained in assisting service professionals to adopt new ways of delivering services [59,60].
Phase V—Build Community-Level Assessment Systems.
As aforementioned, a comprehensive substance use service system requires a monitoring system that would provide information about emerging trends in substances being used, changes in the substance use landscape, and to include systems that assess the link between community service needs and evidence-based programming. Such a system should focus on community-based systems that transfer data to state agencies and ultimately to the national level. These systems should also utilize evidence based methods for implementation readiness [61,62].
Phase VI—Identify Options to Bring the Integrated System of Care Model to Scale.
Communities, especially those already funded and in operation, will benefit from a guidance document drawing from the results of Phases I-VI that delineates how to professionalize and implement a comprehensive substance use service system.
CHALLENGES
The authors are acutely aware of the many challenges to the creation, implementation and sustainability of a community-based comprehensive substance use service delivery system. Vested interests and a culture of ‘this is what we have always done’ or “this cannot be done” will hinder the adoption of the model. In our favor, the results of implementation research studies [61-65], suggest effective methods that can serve to support active and successful implementation.
REFERENCES
- Griffiths P, Vingoe L, Hunt N, Mounteney J, Hartnoll R. Drug information systems, early warning, and new drug trends: can drug monitoring systems become more sensitive to emerging trends in drug consumption? Subst Use Misuse. 2000; 35: 811-44.
- Sloboda Z, Kozel NJ (). Frontline Surveillance: CommunityEpidemiology Work Group for Drug Abuse. In Glantz, MD and Hartel,C. (Eds.) Drug Abuse: Etiology and Interventions, Washington, D.C: APA Press. 1999; 47-62.
- Sloboda Z. Drug abuse epidemiology: An overview. Special Issue of the Bulletin on Narcotics. 2002; LIV. Nos 1 and 2.
- Courtwright D.T. A Century of American Narcotic Policy. In: Gerstein,D.R. & Harwood, H.J. (Eds.) Treating Drug Problems: Volume 2: Commissioned Papers on Historical, Institutional, and Economic Contexts of Drug Treatment. Washington (DC): National Academies Press (US). A Century of American Narcotic Policy. 1992.
- Brook JS, Lukoff IF, Whiteman M. Peer, family, and personality domains as related to adolescents drug behavior. Psychol Rep. 1977; 41: 1095-1102.
- Huba GJ, Wingard JA, Bentler PM. Framework for an interactivetheory of drug use. NIDA Res Monogr. 1980; 30: 95-101.
- Jessor R, Jessor S. A social-psychological framework for studying druguse. NIDA Res Monogr. 1980; 30: 102-109.
- Paton SM, Kandel DB. Psychological factors and adolescent illicit drug use: ethnicity and sex differences. Adolescence. 1978; 13: 187-200.
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychol Bull. 1992; 112: 64-105.
- Chiappini S, Schifano F. An Update on Psychoactive Substances: Pharmacology and Toxicology Issues. Pharmaceuticals (Basel). 2023; 16: 1177.
- Miech RA, Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE, Patrick ME. Monitoring the Future national survey results on drug use, 1975–2019: Volume I, Secondary school students. Ann Arbor: Institute for Social Research, The University of Michigan. 2020.
- Smart R. Natural recovery or recovery without treatment from alcohol and any problems as seen from survey data. In H. Klingemann, & L. Carter-Sobell (Eds.), Promoting self-change from addictive behaviors. New York: Springer. 2007; 59-71
- Sobell LC, Ellingstad TP, Sobell MB. Natural recovery from alcohol and drug problems: methodological review of the research with suggestions for future directions. Addiction. 2000; 95: 749-764.
- Sumnall H, Brotherhood A. Social reintegration and employment: Evidence and interventions for drug users in treatment. EMCDDA Insights Series No 13, Luxembourg: Publications Office of the European Union, 2012, Luxembourg: Publications Office of the European Union. 2012.
- National Research Council. Reducing Risks for Mental Disorders: Frontiers for Preventive Intervention Research. Washington, DC: The National Academies Press. 1994.
- National Research Council and Institute of Medicine. Preventing Mental, Emotional, and Behavioral Disorders among Young People: Progress and Possibilities. Washington, DC: The National Academies Press. 2009
- Xie H, McHugo GJ, Fox MB, Drake RE. Substance abuse relapse in a ten-year prospective follow-up of clients with mental and substance use disorders. Psychiatr Serv. 2005; 56: 1282-1287.
- Rose EJ, Picci G, Fishbein DH. Neurocognitive Precursors of Substance Misuse Corresponding to Risk, Resistance, and Resilience Pathways: Implications for Prevention Science. Front Psychiatry. 2019; 10: 399.
- Lipari RN, Van Horn SL. Children living with parents who have a substance use disorder. The CBHSQ Report. 2017.
- Monitoring the Future. 2022.
- Substance Abuse and Mental Health Services Administration. (2020). Key substance use and mental health indicators in the United States: Results from the 2019 National Survey on Drug Use and Health (HHSPublication No. PEP20-07-01-001, NSDUH Series H-55). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration
- Lappan SN, Brown AW, Hendricks PS. Dropout rates of in-person psychosocial substance use disorder treatments: a systematic review and meta-analysis. Addiction. 2020; 115: 201-217.
- Kozel NJ, Robertson EB, Falkowski CL. The community epidemiologywork group approach. Subst Use Misuse. 2002; 37: 783-803.
- D’Aunno T, Park SE, Pollack HA. Evidence-based treatment for opioid use disorders: A national study of methadone dose levels, 2011-2017. J Subst Abuse Treat. 2019; 96: 18-22.
- Frimpong JA, D’Aunno T, Helleringer S, Metsch LR. Low Rates of Adoption and Implementation of Rapid HIV Testing in Substance Use Disorder Treatment Programs. J Subst Abuse Treat. 2016; 63: 46-53.
- Ringwalt C, Vincus AA, Hanley S, Ennett ST, Bowling JM, Rohrbach LA.The prevalence of evidence-based drug use prevention curricula inU.S. middle schools in 2005. Prev Sci. 2009; 10: 33-40.
- Fishbein DH, Sloboda Z. A National Strategy for Preventing Substance and Opioid Use Disorders Through Evidence-Based Prevention Programming that Fosters Healthy Outcomes in Our Youth. Clin Child Fam Psychol Rev. 2023; 26: 1-16.
- Sloboda Z. Changing patterns of “drug abuse” in the United States: connecting findings from macro- and microepidemiologic studies. Subst Use Misuse. 2002; 37: 1229-1251.
- Madigan S, Racine N, Vaillancourt T, Korczak DJ, Hewitt JMA, Pador P, et al. Changes in Depression and Anxiety Among Children and Adolescents From Before to During the COVID-19 Pandemic: A Systematic Review and Meta-analysis. JAMA Pediatr. 2023; 177: 567-581.
- Albery IP, Mcsweeney T, Hough M. Drug use and criminal behaviour: Indirect, direct or no causal relationship? In J. Adler (Ed.), Forensic psychology: Concepts, debates and practice. Willan Publishing. 2004; 140-156.
- McGovern MP, Carroll KM. Evidence-based practices for substance use disorders. Psychiatr Clin North Am. 2003; 26: 991-1010.
- Sloboda Z, Petras H, Robertson E, Hingson R. (2019). Prevention of Substance Use. Switzerland: Springer Publications. 2019; 133-208.
- United Nations Office on Drugs and Crime. Terminology andInformation on Drugs. 2003.
- International Standards on Drug Abuse Prevention. United Nations Office on Drugs and Crime-World Health Organization. International Standards for the Treatment of Drug Use Disorders. 2020.
- National Academies of Sciences, Engineering, and Medicine. Ending discrimination against people with mental and substance use disorders: The evidence for stigma change.Washington, DC: The National Academies Press. 2016.
- Des Jarlais DC. Harm reduction in the USA: the research perspective and an archive to David Purchase. Harm Reduct J. 2017; 14: 51.
- Levengood TW, Yoon GH, Davoust MJ, Ogden SN, Marshall BDL, Cahill SR et al. Supervised Injection Facilities as Harm Reduction: A Systematic Review. Am J Prev Med. 2021; 61: 738-749.
- Showalter D. Federal funding for syringe exchange in the US: Explaining a long-term policy failure. Int J Drug Policy. 2018; 55: 95- 104.
- Coffin P. Syringe availability as HIV prevention: a review of modalities.J Urban Health. 2000; 77: 306-330.
- Platt L, Minozzi S, Reed J, Vickerman P, Hagan H, French C. Needle andsyringe programmes and opioid substitution therapy for preventing HCV transmission among people who inject drugs: findings from a Cochrane Review and meta-analysis. Addiction. 2018; 113: 545-563.
- Gomez E, Gyger M, Borene S, Klein-Cox A, Denby R, Hunt S, et al. Using SBIRT (Screen, Brief Intervention, and Referral Treatment) Training to Reduce the Stigmatization of Substance Use Disorders Among Students and Practitioners. Subst Abuse. 2023; 17: 11782218221146391.
- Leslie LK, Mehus CJ, Hawkins JD, Boat T, McCabe MA, Barkin S, et al. Primary Health Care: Potential Home for Family-Focused Preventive Interventions. Am J Prev Med. 2016; 51: S106-S118.
- Sloboda Z, Johnson KA, Fishbein DH, Brown CH, Coatsworth JD, Fixsen DL, et al. Normalization of Prevention Principles and Practices to Reduce Substance Use Disorders Through an Integrated Dissemination and Implementation Framework. Prev Sci. 2023; 24: 1078-1090.
- Casey BJ, Cannonier T, Conley MI, Cohen AO, Barch DM, Heitzeg MM, et al. The Adolescent Brain Cognitive Development (ABCD) study: Imaging acquisition across 21 sites. Dev Cogn Neurosci. 2018; 32: 43-54.
- Brown SA, Jernigan TL, Dowling GJ. The adolescent brain cognitivedevelopment study. Health Psychol. 2023; 42: 840-841.
- Jordan CJ, Weiss SRB, Howlett KD, Freund MP. Introduction to the Special Issue on “Informing Longitudinal Studies on the Effects of Maternal Stress and Substance Use on Child Development: Planning for the HEALthy Brain and Child Development (HBCD) Study”. Advers Resil Sci. 2020; 1: 217-221.
- Tai B, Dobbins R, Blackeney Q, Liu D, Moran L. The NIDA clinical trials network: evolving, expanding, and addressing the opioid epidemic. Addict Sci Clin Pract. 2021; 16: 28.
- Substance Abuse and Mental Health Services Administration. Treatment Episode Data Set (TEDS) 2021: Admissions to and Discharges from Substance Use Treatment Services Reported by Single State Agencies. Publication No. PEP23-07-00-004 MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration.2023.
- Lash SJ, Timko C, Curran GM, McKay JR, Burden JL. Implementation of evidence-based substance use disorder continuing care interventions. Psychol Addict Behav. 2011; 25: 238-251.
- Louie E, Barrett EL, Baillie A, Haber P, Morley KC. Implementation of evidence-based practice for alcohol and substance use disorders: protocol for systematic review. Syst Rev. 2020; 9: 25.
- Abraham AJ, Andrews CM, Harris SJ, Friedmann PD. Availability of Medications for the Treatment of Alcohol and Opioid Use Disorder in the USA. Neurotherapeutics. 2020; 17: 55-69.
- Bhad R, Achab S, Rafei P, Kathiresan P, Ardabili HM, Butner J. An online global survey and follow-up expert groups on the scope and needs related to training, research, and mentorship among early- career addiction medicine professionals. Glob Ment Health (Camb). 2023; 10: e44.
- Gleason J. NAACAC’s critical role in the development of a profession:40 years of achievement. Advances in Addictions and Recovery. 2014; 8-17.
- Kerwin ME, Walker-Smith K, Kirby KC. Comparative analysis of state requirements for the training of substance abuse and mental health counselors. J Subst Abuse Treat. 2006; 30: 173-181.
- Olmstead TA, Abraham AJ, Martino S, Roman PM. Counselor training in several evidence-based psychosocial addiction treatments in private US substance abuse treatment centers. Drug Alcohol Depend. 2012; 120: 149-154.
- Roman PM, Abraham AJ, Knudsen HK. Using medication-assisted treatment for substance use disorders: evidence of barriers and facilitators of implementation. Addict Behav. 2011; 36: 584-589.
- Hogue A, Brykman K, Guilamo-Ramos V, Ilakkuvan V, Kuklinski MR, Matson P, et al. Family-Focused Universal Substance Use Prevention in Primary Care: Advancing a Pragmatic National Healthcare Agenda. Prev Sci. 2024; 25: 307-317.
- Matson PA, Ridenour T, Ialongo N, Spoth R, Prado G, Hammond CJ et al. State of the Art in Substance Use Prevention and Early Intervention: Applications to Pediatric Primary Care Settings. Prev Sci. 2022; 23: 204-211.
- Aijaz M, Fixsen D, Schultes MT, Van Dyke M. Using Implementation Teams to Inform a More Effective Response to Future Pandemics. Public Health Rep. 2021; 136: 269-273.
- Schultes MT, Aijaz M, Klug J, Fixsen DL. Competences for implementation science: what trainees need to learn and where they learn it. Adv Health Sci Educ Theory Pract. 2021; 26: 19-35.
- Chinman M, Ebener P, Malone PS, Cannon J, D’Amico EJ, Acosta J. Testing implementation support for evidence-based programs in community settings: a replication cluster-randomized trial of Getting To Outcomes®. Implement Sci. 2018; 13: 131.
- Johnson K, Collins D, Wandersman A. Developing a sustainability readiness strategy for health systems: Toolkit, interactive tools, and virtual support system. Eval Program Plann. 2023; 97: 102241.
- Fixsen DL, Blase KA. The Teaching-Family Model: The First 50 Years.Perspect Behav Sci. 2018; 42: 189-211.
- D’Aunno T. The role of organization and management in substance abuse treatment: Review and roadmap. J Subst Abuse Treat. 2006; 31: 221-233.
- Hall OT, Hall OE, Kolodny A, Teater J, McGrath RP. Assessment of Excess Mortality Associated With Drug Overdose in Ohio From 2009 to 2018. JAMA Netw Open. 2020; 3: e202183.










































































































































{kind=link}