A Case of Oropharyngeal Chordoma
- 1. Department of ENT, Universitary Hsopital of Annaba, University Badji Mokhtar, Algeria
Abstract
Chordomas are rare malignant neoplasms derived from incomplete regression of notochordal tissue along the cranio-coccygeal axis. We report a case of retropharyngeal chordoma presenting with dysphagia and operated on by trans oral approach associated a post-operative radiotherapy. Chordomas must to be evocated in retrophayngeal tumors required a good checking (imaging, cytology) and conformed by immunohistological exam. The prognosis is poor.
Keywords
- Retropharyngeal tumor; Chordoma; Trans oral surgery
Citation
Kharoubi S (2025) A Case of Oropharyngeal Chordoma. Ann Otolaryngol Rhinol 12(6): 1378.
INTRODUCTION
Chordoma is a rare malignant bone tumor that can arise anywhere along the central neural axis. This tumor is derived from remnants of the notochord an embryogenic structure that is required for the induction of the neural plate in the embryogenic disk. The majority of chordomas arise at the skull base and a minority along the cervical spine. Extra-axial locations have been reported in the head and neck including the nasopharynx, paranasal sinuses, lateral nasal wall, oropharyngeal and soft tissue of the neck. Chordomas tend to be slow-growing without specific symptoms. Diagnosis is facilitated by imaging (CT scan, MRI). The management of chordomas is complex (surgical procedure and post operative radiotherapy) with poor prognosis (local recurrence and metastasis). Genetic research (mutations) and target therapy may be ameliorating the evolutivity of these tumors. In reality, the most challenging aspect of this pathology is requiring a pre-operative diagnosis of chordoma because it facilitates management especially surgical approaches (trans oral, external) and quality of resection (capsule effraction, residual tumor).
CASE PRESENTATION
71-year-old women consulted with medial dysphagia during 13 months. She reported a foreign body sensation and actually the perturbance was important and imposed a modification of food ingrain (liquid foods). The global status of this patient is good (memory, hemodynamic constants, cardiac and renal functions). She reports an amigrissement of 8 kg without perturbance (asthenia). Clinical exam revealed a 5 X 4 cm mass in the posterior part of oropharyngeal way. Mucous was well without ulceration. Palpation was not pulsate and not painful. Fibroscopy not shows a nasopharyngeal or hypo pharyngeal extension. The lesion was strictly medial without lateral (para pharyngeal extension). Cervical and cranial nerve evaluation was normally. Enhanced computed tomography showed limited tumor of oropharyngeal space (Figure 1,2).

Figure 1 Sagittal CT scan, retropharyngeal tumor with oropharyngeal expression.
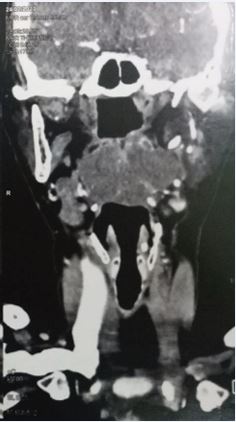
Figure 2 Coronal CT scan, retropharyngeal tumor with oropharyngeal expression.
MRI revealed a 5X4, 5 cm mass occupied retro oropharyngeal space without osteolysis (cervical spine) (Figure 3,4).
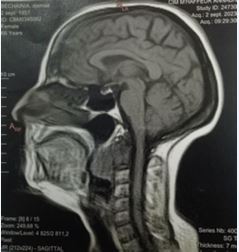
Figure 3 Sagittal MRI retropharyngeal tumor encapsulated hyposignal T1.
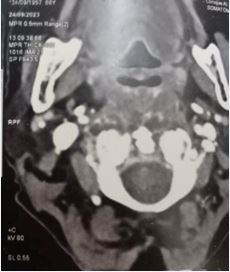
Figure 4 Axial MRI retropharyngeal tumor with calcification.
Cytologic speed cell was not contributive. The patient conferment surgery via the trans oral approach. After vertical incision and posterior muscular dissection, we found a no capsular tumor, greyish poorly hemorrhagic. A dissection was made by progressively cliving the mass to vertebral spine. After removing the operative site was vide without hemorragy. We sutured the muscular part (vicryl 2/0) with safety following. The anatomopathological exam of specimen after immunohistochemistry testing revealed chordoma (conventional subtype) (Figure 5). Post operative radiotherapy is occurred and follow – up after 15 months is safety.
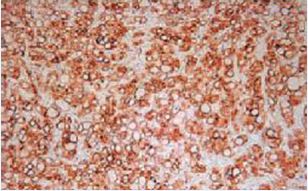
Figure 5 Chordoma: immunohistochemical staining: positive reaction to cytokeratin.
DISCUSSION
Chordoma incidence actually is 8 per 100 000 population [1]. It was first described by Lusschain 1857 [2]. It arises from notocord tissue and occurs along the cranio coccygeal axis. Studies report 50% of chordomas occur in the sacro-coccygeal region, 35% in the spheno-occipital region, and 15% in the spine [3]. Chordoma interesting adults with a median age of 51 years patients but it can be seen in 4 to 80 years. Males and females are affected equally and head and neck chordomas tend to present one decade earliery than other sites.
The symptoms in oropharyngeal chordoma may include dysphagia, foreign body sensation, snoring, rhinolalia and sleep-apnea. Dysphonia, nasal obstruction and ever dyspnea can be seen in nasopharyngeal or hypo pharyngeal location.
Clinical exam shows a mass (variable dimension) in oropharyngeal wall (retropharyngeal space) recovered by normal mucosa aspect (broken or bleeding mucosa is rare). CT scan is the first imaging exam. He shows the mass (location) and authorizes mensuration, extension, vascular characterization, and cervical spine reaction (lysis). In MRI, the chordoma signals are commonly iso intense or hypo intense on T1-weighted images and hyper intense on T2-weighted images.
Fine needle aspiration biopsy may be helpful for pre operative diagnosis. The WHO classification recognizes three chordomas subtypes: conventional, dedifferentiated and poorly differentiated chordomas. Histopathological exam for chordoma shows a lobulated mass with a gelatinous or chondroid cut surface. Microscopically chondroma is composed of cords of tumor cells embedded within a myxoid materix and arranged in lobules separated by fibrous septa. Chordomas sub types include chondroid chordoma, cellular chordoma, poorly differentiated chordoma and dedifferentiated chordoma. Immunochemistry straining of chordoma is positive for cytokeratin, epithelial membrane antigen (EMA) and S-100 protein.
Genetic alteration: Genetically, chordomas are notable for the loss of CDKN2A and PTEN expression and large copy number losses, particulary in chromosomes 1p,3,9,10,13,14, and 18 [4]. Differential diagnoses include neurogenic tumors, lymphoma, chondrosarcoma, meningioma, myoepithelial carcinoma, glioma. The evolution of chordomas is poor. Median survival with chordoma is 6,3 years, though is just 16 months in dedifferentiated choroma [1]. Chordomas most commonly metastasize to the lung, lymph nodes, bone, liver and subcutaneous tissues [5,6]. The gold standard treatment of chordomas is surgical resection followed by post operative radiotherapy. Complete resection is necessary followed by post operative radiotherapy. Complete resection is, necessary because of the malignant nature of chordomas. The tumor capsule will be considered because if she is broken the tumor will aggressively recur. Complete resection is only achieved in 29% of cases [6,7].
The location and extension of the tumor influenced the surgical approach. The trans oral procedure is recommended in little tumors (over to 35 mm) without para pharyngeal or skull base extension removing in good condition is possible (capsule). The use of coablation or sheaver can to be facilitate the surgery. Reconstruction of muscular part of retropharyngeal space achieves a poor morbidity. All other cases may be treated by external approach; lateraly cervical incision, dissection and safety protect the vascular pedicle of the neck, Identifying the vagus nerf, retropharyngeal muscular incision and exposition of the cervical spine and exploring the lesion.
Trans oral robotic surgeryis an appreciable and safe procedure in oropharyngeal chordomas. Chordomas are not sensitive to chemotherapy. Some studies assessing the efficacy of EGFR inhibitors (imatinib) in locally advanced and metastatic chordoma [8]. The post-operative imaging (CT-scan, MRI) is an appreciate step to evaluate the quality (total or not) of surgical resection and may be helpful for the follow-up of patients (persistence disease or recurrence). The prognosis of chordoma depends on age (under 5 years or over 50 years), site, mensurations (superior to 4.0 cm), local extension, quality of surgical resection (capsule), and histological sub type (better prognosis of chondroid chordoma). The 5-year survival rate is only 20% and the median survival duration is only 4,1 years [9].
CONCLUSION
Chordoma is a malignant tumor of notochord origin that can arise in head and neck locations with variable management difficulties. Imaging is a very important step for diagnosis and protocol therapy proposing. Surgery is required in all cases with variable difficulties (quality of resection) associated with post-operative radiotherapy. Genetic and pharmacological (target therapy) research can ameliorate in the future the management and the prognosis of chordomas.
REFERENCES
- McMaster ML, Goldstein AM, Bromley CM, Ishibe N, Parry DM. Chordoma: Incidence and survival patterns in the states, 1973 1995 Cancer Causes Control. 2001; 12: 1-11.
- Friedmann I, Harrision DF, Bird ES. The fine structure of chordoma with particular reference to the physaliphorous cell. J Clin Pathol. 1962; 15: 116-125.
- Sundersan N, Galicich JH, Chu FC. Spinal chordomas. J Neurosurg. 1979; 50: 312-319.
- Le LP, Nielsen GP, Rosenberg AE, Thomas D, Batten JM, Deshpande V, et al. Recurrent chromosomal copy number alterations in sporadic chrdomas PloS ONE. 2011; 6: e18846.
- Jo VY, Fletcher CD. CDMWorld Health Organization. International Agency for Research on cancer.2013 WHO classification of tumours of soft tissue and bone. IARC Press Lyon. 2014; 46: 95-104.
- Wasserman JK, Gravel D, Purgina B. Chordoma of the head and neck: a review. Head and Neck Pathol. 2018; 12: 261-268.
- Bohman LE, Koch M, Bailey RL, Alonso-Basanta M, Lee JY. Skull base chordoma and chondrosarcoma influence of clinical and demographic fators on prognosis: a SEER analysis. World Neurosurg. 2014; 82: 806-814.
- Hindi N, Casali PG, Morosi C, Messina A, Palassini E, Pilotti S, et al. Imatinib in advanced chordoma: a retrospective case series analysis. Eur J Cancer. 2015; 51: 2609-2614.
- Gladstone HB, Bailet JW, Rowland JP. Chordoma of the oropharynx, an unusual presentation and review of the literature. Otolaryngol Head Neck Surg. 1998; 118: 104-107.








































































































































