A Pediatric Case of Bilateral Custom Made Prostheses of TMJ and Literature Review
- 1. University of L’Aquila, Italy
Abstract
Introduction: Temporomandibular Joint Ankylosis (TMJA) is a pathological condition characterized by limitation of the opening of the mouth caused primary by trauma but also by infection, inflammatory and congenital diseases. TMJA can be treated through the utilization of autogenous grafts or alloplastic TMJ prostheses. There are two types of alloplastic TMJ prostheses: stock or custom. In the last years custom alloplastic TMJ prostheses are the emerging treatment modality for TMJ ankylosis.
Presentation of the case: A 16-year-old male patient presented with a 1 cm interincisal opening for about 2 years and inability to chew and speak. He referred ankylosis appeared after a trauma. The ankylotic masses were of 17,6 mm on the right side and 19,6 mm on the left side. A bilateral removal of the ankylosis and a custom-made prostheses reconstruction was programmed.
Clinical discussion: Treatment options for TMJ ankylosis are various. Stock alloplastic TMJ prostheses may not suit all patients due to anatomical variations. Thus, custom alloplastic TMJ prostheses have emerged as the preferred treatment modality for TMJ ankylosis. We also conducted a review of the literature regarding patients who underwent bilateral custom-made prostheses. This treatment
Conclusion: Custom alloplastic TMJ prostheses are considered an optimal treatment modality for reconstructing the TMJ in adult and young adult patients with TMJ ankylosis. The implantation of custom-made prostheses is not associated with any peri- and postoperative complications.
Keywords
• TMJ; Ankylosis; Custom Made Prostheses; Maxillo Facial Reconstruction
Citation
Lupi E (2025) A Pediatric Case of Bilateral Custom Made Prostheses of TMJ and Literature Review. Ann Otolaryngol Rhinol 12(6): 1376.
INTRODUCTION
Temporomandibular Joint Ankylosis (TMJA) is defined as a permanent constriction of the jaws with MIO (Maximal Incisal Opening) less than 30 mm between the incisors, occurring because of bony, fibrous or fibro-osseous fusion of the mandibular condyle with the temporal bone fossa. This pathological condition causes chewing, swallowing, speech, oral hygiene, airway function impediment and impaired quality of life [1,2]. Trauma is the main etiology for the occurrence of temporomandibular joint ankylosis [3-5].
Other causes can be infection, inflammatory disease (such as rheumatoid arthritis and ankylosing spondylitis) and more rarely congenital diseases. The treatment for TMJA can be an autogenous graft or alloplastic prosthesis. Complication of autogenous grafts is potential resorption, donor site morbidity, increased surgical time and graft fracture. Alloplastic TMJ prostheses can be both custom and stock. The former are emerging as the preferred treatment choice for adults affected by TMJA [2-6].
Perpetual failure rates with re-ankylosis and inability to maintain long term mouth opening, has been a challenge in management of TMJA. A higher percentage of cases of TMJA is found in many developing countries because of the lack of adequate access to healthcare and unavailability of surgical expertise. Some reports show that often patients seek treatment for ankylosis problems years after onset of symptoms [7].
If ankylosis develops during childhood, it results in severe mandibular growth retardation. Involvement of one joint can lead to facial asymmetry. Instead, the involvement of both the joints can lead to mandibular undergrowth and respiratory problems. A 16-year-old male patient, presented with a complete inability to open his mouth, chew or speak for the last 2 years. His diet was totally based on liquid food. On objective inspection, a limited mouth opening with an interincisive distance of about 1 cm was observed. The work has been reported in line with the SCARE criteria.
PRESENTATION OF THE CASE
A 16-year-old male patient presented to Maxillofacial Unit of San Salvatore Hospital University of L’Aquila in November 2022 for limitation and pain at mouth opening and dental abscess. The patient reports being a victim of facial trauma about 2 years before and noticing in the following months a gradual reduction in mouth opening and the onset of pain at the temporomandibular joint bilaterally. The patient reported increased pain at night, which he treated by taking daily multiple pain medications. On inspectional facial physical examination, no asymmetries were evident. A swelling given by dental abscess was observed. On physical examination, the patient presented a retruded facial profile. When asked to open the mouth, the maximum interincisive distance was about 1 cm. On palpatory objective examination of the TMJ, no joint movement was perceptible. Intraoral examination was difficult to perform because of the limited mouth opening. Numerous decayed teeth were observed on both arches. The patient underwent a facial CT scan showing bilateral ankylosis between the mandibular condyle and glenoid fossa of the temporalis bone. Reduced growth of the mandibular ramus was also observed. Numerous carious tooth elements were also present. On objective inspection, a sternal manubrium deformity was also observed to be related to an another mal-consolidated fracture outcome. The patient did not refer other comorbidities. Our team subjected the patient to antibiotic treatment to resolve the dental abscess. Surgical indication was also given for removal of the ankylotic blocks bilaterally. Preoperative routine baseline blood investigations, Electrocardiogram (ECG) and viral marker testing were conducted with all the results falling within the normal range (Figure 1).
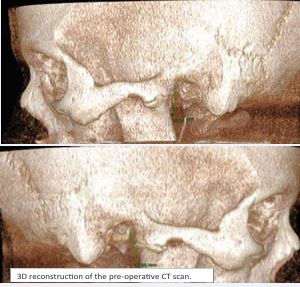
Figure 1 3D reconstruction of the pre-operative CT scan.
VIRTUAL SURGICAL TREATMENT PLANNING
The main purpose of surgical treatment was to restore a normal mouth opening. Our surgical planning was based on facial CT scan. Considered the dimension of ankylosis, we planned on the right side an inferior osteotomy about 1,8 cm above the right mandibular angle and on the left side about 1,6 cm above the left mandibular angle. The superior osteotomy was performed below the zygomatic arch. On both sides coronoid process was removed. The dimension of the ankylotic masses on the right side is about 17,6 mm, on the left side is 19,6 mm (Figure 2).

Figure 2 Preoperative MIO of the patient.
In order to realize a most specific treatment, cutting guides and customized components were fabricated by engineers for the bilateral reconstruction of the new TMJ. The customized prosthesis was made of two distinct parts: the fossa component and the ramus-condyle unit. The fossa and the condyle were composed of titanium, between these two parts was positioned an insert made of polyethylene.
Surgery
The patient was positioned supine for the procedure. Before the beginning of the surgery a tracheotomy was performed under local anesthesia because of the reduced mouth opening. Preauricolar pretragic incision and submandibular incision were performed bilaterally. After identification and dissection of the ankylotic mass from the surrounding tissues, cutting dice were placed to perform the excision. The facial nerve was preserved bilaterally. The gap between the zygomatic arch and the mandibular ramus was about 2 cm. Before the insetting of the glenoid fossa prosthesis the polyethylene insert was applied. Then the glenoid fossa was fixed to the zygomatic arch with four screws on both sides. The condyle was inserted from the submandibular incision and after ascertaining the proper relationship with the fossa, it was fixed with 7 screws bilaterally. Hemostasis was achieved and primary closure was done after thorough irrigation. At the end of surgery, compression medication was performed to prevent hematoma.
The patient spent the first night in the sedated ICU postoperatively. The patient was extubated on the first post-operative day. On the same day a CT scan of the face was performed. After 5 days, the tracheotomy cannula was removed. The patient suffered neither facial nerve damage nor damage to the inferior alveolar nerve. The patient was discharged on the ninth postoperative day. The patient started passive physiotherapy 2 weeks after surgery. At three months after surgery, he is still doing active and passive physical therapy Figure 3).

Figure 3 Post-operative MIO is about 3 cm.
DISCUSSION
The aim of this case was to restore a normal buccal motility and to correct the facial deformity in a child with bilateral TMJA using custom alloplastic TMJ prosthesis. Alloplastic joint replacement is well documented in orthopedics [7-9]. TMJ like all other joints like knee and hip can be affected by joint disorders making the replacement of joint a necessity.
The decision to use a custom-made prosthesis was based on several factors. Primarily, the fact that this type of procedure is associated with a low complication rate. Dimitroulis observed that placement of autogenous tissue such as bone into an area where reactive or heterotopic bone is forming leads to further ankylosis.
They suggest the use of total TMJ prosthesis in re-ankylosis cases [10]. As reported in 2014 by Wolford and Mercuri [11], in a cohort of 56 patients undergoing custom-made temporomandibular joint prostheses, none showed complications. The ability to use cutting templates allows for more precise osteotomies. The phantoms used in resection of the ankylotic block also have guides for the screws of the prosthesis; this reduces the surgical time for fixation of the prosthesis themselves. In addition, when autogenous grafts are used, possible donor site complications must also be considered. Multiple studies have consistently demonstrated the achievement of adequate mouth opening through the utilization of alloplastic TMJ [11-15].
According to some studies heterotopic bone formation can cause recurrence of TMJA. For this reason, they recommend placing abdominal fat pad or fascia lata graft surrounding the alloplastic TMJ. In our case we did not use fat pad [16,17]. Both the ramus-condyle unit and the fossa component of the custom alloplastic Temporomandibular Joint (TMJ) are fabricated using titanium, while the insert between these two parts is composed of Ultra-High Molecular Weight Polyethylene (UHMWPE). Mercuri and Caicedo created a protocol for the management of material hypersensitivity [18]. They advised to take an appropriate previous history of allergy to any metal preoperatively. If an allergy is reported an allergen-free prosthesis should be considered. Postoperatively, if symptoms appear, if all the other possible reasons are excluded and metal hypersensitivity is detected, blood analysis is advised. If the test is positive, the explantation is mandatory. Westermark has reported that modern TMJ prosthesis (with condyle made up of Co Cr–Mo and fossa made up of UHMWPE) function without foreign body reaction [16]. However, according to Mercuri [16], the incidence of reactions is lower in metal on UHMWPE compared to metal-on-metal configurations. For this reason, we decided, in consultation with engineers, to choose this type of prosthesis.
Coronoidectomy is usually performed in TMJ replacement. The absence of coronoid process can lead to dislocation of prosthesis especially when it is performed bilaterally [19-21]. An accurate alignment of mandibular component is important to avoid dislocation of prosthesis head [22]. According to Mustafa and Sidebottom the patient should be kept on light elastics for one week to prevent postoperative dislocation [23]. Relocation of the joint prosthesis is easier in these patients as compared to normal patients. We also decided to remove the coronoid process bilaterally to simplify the prostheses implantation. Prevention of Periprosthetic Joint Infections (PJIs) is very important as the management of PJIs is a difficult task. PJIs have been reported after the use of alloplastic TJR [24]. In our case we administered for a10 days 3 gr daily of amoxicillin/ clavulanic acid. This clinical case highlights the success achieved in restoring normal mouth opening in an adolescent. At present, 3 months after surgery, the MIO is reported to be 3 cm. This result was achieved without any complications. We conducted a review by collecting cases reported in the literature of temporomandibular joint ankylosis treated surgically with the placement of custom-made prostheses [25-31]. We selected eight articles. We could find that most of articles in the literature are on monochondylar treatments and performed with stock prostheses. The patient group gathered from studies in the literature consists of 17 people, 8 males and 9 females. The average age is 25, 1 years, with a range of 14 to 58 years. The patients in our group were treated between 2003 and 2023 (Table 1).
Table 1: 17 Collected cases reported in the literature of temporomandibular joint ankylosis treated surgically with the placement of custom-made prostheses.
|
Patient |
Age |
MIO (mm) |
Physiotherapy |
|
1 |
47 |
30 |
No |
|
2 |
19 |
23 |
Yes |
|
3 |
18 |
25 |
Yes |
|
4 |
14 |
30 |
Yes |
|
5 |
14 |
25 |
Yes |
|
6 |
16 |
30 |
Yes |
|
7 |
14 |
28 |
No |
|
8 |
17 |
40 |
Yes |
|
9 |
58 |
27 |
Yes |
|
10 |
24 |
27 |
Yes |
|
11 |
21 |
27 |
Yes |
|
12 |
24 |
27 |
Yes |
|
13 |
22 |
27 |
Yes |
|
14 |
22 |
27 |
Yes |
|
15 |
25 |
27 |
Yes |
|
16 |
51 |
41 |
No |
|
17 |
20 |
38 |
Yes |
Inclusion criteria are: removal of ankylotic block bilaterally and reconstruction of TMJ using custom-made prosthesis. Only one patient had undergone previous arthroplasty and temporalis muscle flap surgery and 10 years later underwent prosthesis.
Out of 17 patients, only two reported postoperative complications. These complications resulted in facial nerve damage. One patient had permanent damage of the temporal branch of the facial nerve. Another one had a partial deficit of the zygomatic branch, which resolved spontaneously after 1 month. No other complications were observed.Of 17 patients, 14 of them started active and passive physiotherapy between postoperative weeks 1 and 4. The cause of ankylosis found in all patients was related to facial trauma, especially during childhood or adolescence. The average MIO in the immediate postoperative period is 29.3 mm. Data regarding long-term follow-up are lacking.
Based on our review, we can assert that our result is in line with those obtained by colleagues in other countries. The implantation of custom-made prostheses is not associated with any peri- and postoperative complications, is well suited for young patients, and allows recovery of excellent mandibular kinetic function. An important challenge to consider will be that related to the need to change prostheses considering the young age of the patients. Regarding this issue, we found no relevant reports in the literature.
CONCLUSION
Comparing our case with cases found in the literature who underwent the same procedure, we note similarities such as young age, cause of ankylosis and the low rate of postoperative complications. Our follow-up is currently limited being less than 4 months after surgery.
ACKNOWLEDGMENTS
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript. Apart from patient’s personal data, data sharing is not applicable to this article as no new data were created or analyzed in this study.
REFERENCES
- Bénateau H, Chatellier A, Caillot A, Diep D, Kün-Darbois JD, Veyssière A. L’ankylose temporo-mandibulaire [Temporo-mandibular ankylosis]. Rev Stomatol Chir Maxillofac Chir Orale. 2016; 117: 245-255.
- Adhikari M, Upadhyaya C, Jha K, Adhikari G. Management of bilateral temporomandibular joint ankylosis using bilateral custom alloplastic temporomandibular joint prosthesis and genioplasty: A case report. Int J Surg Case Rep. 2023; 109: 108516.
- Bhatt K, Roychoudhury A, Bhutia O, Pandey RM. Functional outcomes of gap and interposition arthroplasty in the treatment of temporomandibular joint ankylosis. J Oral Maxillofac Surg. 2014; 72: 2434-2439.
- Roychoudhury A, Yadav P, Alagarsamy R, Bhutia O, Goswami D. Outcome of Stock Total Joint Replacement With Fat Grafting in Adult Temporomandibular Joint Ankylosis Patients. J Oral Maxillofac Surg. 2021; 79: 75-87.
- Roychoudhury A, Parkash H, Trikha A. Functional restoration by gap arthroplasty in temporomandibular joint ankylosis: a report of 50 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87: 166-169.
- Roychoudhury A, Yadav P, Bhutia O, Mane R, Yadav R, Goswami D, et al. Alloplastic total joint replacement in management of temporomandibular joint ankylosis. J Oral Biol Craniofac Res. 2021; 11: 457-465.
- Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007; 370: 1508-1519.
- NICE. Total hip replacement and resurfacing arthroplasty for end stage arthritis of the hip. NICE technology appraisal guidance 304. National Institute for Health and Care Excellence, London. 2014.
- Evans JT, Evans JP, Walker RW, Blom AW, Whitehouse MR, Sayers A. How long does a hip replacement last? A systematic review and meta- analysis of case series and national registry reports with more than 15 years of follow-up. Lancet. 2019; 393: 647-654.
- Dimitroulis G. Temporomandibular Joint Surgery: What Does it Mean to India in the 21st Century? J Maxillofac Oral Surg. 2012; 11: 249- 257.
- Roychoudhury A, Yadav P, Alagarsamy R, Bhutia O, Goswami D. Outcome of Stock Total Joint Replacement With Fat Grafting in Adult Temporomandibular Joint Ankylosis Patients. J Oral Maxillofac Surg. 2021; 79: 75-87.
- Sohrabi C, Mathew G, Maria N, Kerwan A, Franchi T, Agha RA; Collaborators. The SCARE 2023 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg. 2023; 109: 1136- 1140.
- Wolford LM, Mercuri LG, Schneiderman ED, Movahed R, Allen W. Twenty-year follow-up study on a patient-fitted temporomandibular joint prosthesis: the Techmedica/TMJ Concepts device. J Oral Maxillofac Surg. 2015; 73: 952-960.
- Mercuri LG. A rationale for total alloplastic temporomandibular joint reconstruction in the management of idiopathic/progressive condylar resorption. J Oral Maxillofac Surg. 2007; 65: 1600-1609.
- Sidebottom AJ, Gruber E. One-year prospective outcome analysis and complications following total replacement of the temporomandibular joint with the TMJ Concepts system. Br J Oral Maxillofac Surg. 2013; 51: 620-624.
- Wolford LM, Morales-Ryan CA, Morales PG, Cassano DS. Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone formation. Proc (Bayl Univ Med Cent). 2008; 21: 248-254.
- Giovannetti F, Barbera G, Priore P, Pucci R, Della Monaca M, ValentiniV. Fascia Lata Harvesting: The Donor Site Closure Morbidity. J Craniofac Surg. 2019; 30: e303-e306.
- Mercuri LG, Caicedo MS. Material Hypersensitivity and Alloplastic Temporomandibular Joint Replacement. J Oral Maxillofac Surg. 2019; 77: 1371-1376.
- Westermark A. Total reconstruction of the temporomandibular joint. Up to 8 years of follow-up of patients treated with Biomet(®) total joint prostheses. Int J Oral Maxillofac Surg. 2010; 39: 951-955.
- Gruber EA, McCullough J, Sidebottom AJ. Medium-term outcomes and complications after total replacement of the temporomandibular joint. Prospective outcome analysis after 3 and 5 years. Br J Oral Maxillofac Surg. 2015; 53: 412-425.
- Murdoch B, Buchanan J, Cliff J. Temporomandibular joint replacement: a New Zealand perspective. Int J Oral Maxillofac Surg. 2014; 43: 595- 599.
- Mercuri GL. The role of custom-made prosthesis for temporomandibular joint replacement. Revista Española de Cirugía Oral y Maxilofacial. 2013; 35: 1-10.
- Mustafa el M, Sidebottom A. Risk factors for intraoperative dislocation of the total temporomandibular joint replacement and its management. Br J Oral Maxillofac Surg. 2014; 52: 190-192.
- Mercuri LG, Psutka D. Perioperative, postoperative, and prophylactic use of antibiotics in alloplastic total temporomandibular joint replacement surgery: a survey and preliminary guidelines. J Oral Maxillofac Surg. 2011; 69: 2106-2111.
- Yadav P, Roychoudhury A, Kumar RD, Bhutia O, Bhutia T, Aggarwal B. Total Alloplastic Temporomandibular Joint Replacement. J Maxillofac Oral Surg. 2021; 20: 515-526.
- Neelakandan RS, Raja AV, Krishnan AM. Total Alloplastic Temporomandibular Joint Reconstruction for Management of TMJ Ankylosis. J Maxillofac Oral Surg. 2014; 13: 575-582.
- Gerbino G, Zavattero E, Berrone S, Ramieri G. One stage treatment of temporomandibular joint complete bony ankylosis using total joint replacement. J Craniomaxillofac Surg. 2016; 44: 487-492.
- Adhikari M, Upadhyaya C, Jha K, Adhikari G. Management of bilateral temporomandibular joint ankylosis using bilateral custom alloplastic temporomandibular joint prosthesis and genioplasty: A case report. Int J Surg Case Rep. 2023; 109: 108516.
- Keyser BR, Banda AK, Mercuri LG, Warburton G, Sullivan SM. Alloplastic total temporomandibular joint replacement in skeletally immature patients: a pilot survey. Int J Oral Maxillofac Surg. 2020; 49: 1202-1209.
- Val M, Ragazzo M, Bendini M, Manfredini D, Trojan D, Guarda Nardini L. Computer-assisted surgery with custom prostheses and human amniotic membrane in a patient with bilateral class IV TMJ reankylosis: a case report. Cell Tissue Bank. 2022; 23: 395-400.
- Mommers XA, Wajszczjak L, Zwetyenga N. Résultats fonctionnels après reconstruction de l’articulation temporo-mandibulaire par prothèse totale (2e partie) [Functional results after temporomandibular joint reconstruction using a total joint prosthesis (part II)]. Rev Stomatol Chir Maxillofac Chir Orale. 2014; 115: 10-14. French.








































































































































