Esthesioneuroblastoma: About 12 Cases
- 1. Department of General Surgery, General Hospital of Tianjin Medical University, China
Abstract
Esthesioneuroblastoma (ENB) is a rare malignant tumor developed at the expense of the neuro-olfactory epithelium, and is among the rarest of nasal cavity tumors. It is often manifested by rhinological signs, the ocular damage may be inaugural or appears during the evolution of the secondary orbital damage. Computed tomography and magnetic resonance imaging allow a very precise local and general assessment. The diagnosis is anatomo -pathological and treatment usually relies on surgery and radiotherapy.
Methods: Retrospective study of 12 cases within ENT department of the CHU HASSAN II of FEZ over a period of 10 years.
Results: The average age of our patients was 45 years with no clear gender predominance. The average consultation time was 8 months. Rhinosinus syndrome was the predominant sign of clinical symptomatology, sometimes associated with ophthalmologic or neurological signs. All our patients benefited from a radiological assessment that allowed to highlight the tumour as well as its locoregional extensions. Four cases of intracranial expansion were detected. Of the 12 cases, 10 patients received surgical management (either endonasal alone in six cases, combined in three cases, or external alone (paralateronasal type of Moure) in a single patient) followed by complementary radiotherapy. Evolution has been satisfactory. In the remaining 2 cases, treatment was only palliative (chemotherapy or radiotherapy) due to the extension of the tumor.
Conclusion: Esthesioneuroblastoma (ENB) is a rare tumour, first described by Berger in 1924, it mainly affects humans and occurs most often during the second and third decades. Clinical revealing manifestations are dominated by rhinological signs (uniform or bilateral nasal obstruction, epistaxis, anosmia). Neurological signs are common and ophthalmologic manifestations, such as exophthalmia, reflect tumor expansion at the orbital level. The precise diagnosis can only be made by anatomopathology. Treatment is based on surgical removal combined with radio chemotherapy.
Keywords
- Esthesioneuroblastoma; Malignant tumor; Nasal cavity tumors; Humans
Citation
Adoua Y, Maqboub O, Ouahidi Y, Oudidi A, Benmansour N, et al. (2024) Esthesioneuroblastoma: About 12 Cases. Ann Otolaryngol Rhinol 11(3): 1338.
INTRODUCTION
Esthesioneuroblastoma or olfactory neuroblastoma is a rare malignant tumour of the nasal cavities, developed at the expense of the olfactory epithelium [1,2]. Since its first description by Berger and Luc in 1924 as olfactory esthesioneuroepitheluim [3]. Limited series have been reported in the literature reflecting the difficulties of positive diagnosis.
Through a retrospective study for 10 years between 2014 and 2024, we will analyze a series of 12 patients with Esthesioneuroblastoma who were collected at the ENT department of the CHU Hassan II of Fez.
The objective of our work is to study the different epidemiological, clinical and therapeutic parameters of this disease, then we propose to take stock of the etiopathogenic hypotheses, the diagnostic means and the therapeutic modalities available to us for the management of these tumors.
MATERIALS AND METHODS
This is a retrospective study spanned 10 years between 2014 and 2024, involving 12 patients from the ORL service of the CHU Hassan II of Fez. Cases included in our study are patients, men and women of all ages, who have been seen and treated for Esthesioneuroblastoma at the ENT department of the CHU Hassan II of Fez.
RESULTS
Between 2014 and 2024, we had the opportunity to treat 12 cases of esthesioneuroblastoma. There were 5 men and 7 women. The age ranged from 26 to 70 years with a mean of 48 years. The average consultation time was 8 months with extremes ranging from 2 months to 14 months. Call signs were mainly nasal obstruction and epistaxis present in all patients followed by anosmia, swelling of the face and rhinorrhea in half of the cases. On the other hand, ophthalmologic signs were observed in three cases.
Clinical examination via the Endoscopy revealed the tumour and did the biopsy that confirmed the diagnosis (Figure 1).

Figure 1: Endoscopic aspect of a budding process of the left FN. (Iconography of the service)
The radiological assessment (CT and/or MRI) revealed the tumour and its locoregional extensions. Two cases of intracranial expansion have been identified (Figure 2).

Figure 2: Axial facial CT showing left naso-ethmoidal heterogeneous process and tissue density with endocranial extension and towards the homolateral orbit. (Iconography of the service)
A remote extension assessment was performed in all our patients to establish a TNM classification: the majority of our patients were classified between T2 and T3 (6 cases), 2 cases of T1 and 4 patients with a tumour classified as T4. Cervical lymphadenopathy was found in 2 cases and distant metastases in only one case.
Of the 12 cases, 10 patients received curative treatment (first surgery followed by radiotherapy of 50-60Gy) or endonasal treatment in 6 patients, followed by paralateronasal of Moure in a single patient or combined in 3 cases. For the remaining 2 patients the lesion was so explosive with invasion of the neighboring structures that they were offered a palliative treatment: chemotherapy included cyclophosphamide (650 mg/ m2) with vincristine (1. 5 mg/m2 with a maximum dose of 2 mg/ m2) (Table 1) (Figure 3).
Table 1: The majority of our patients had a positive development, with a 5 year decline.
|
case |
age |
sex |
Consultation time |
clinical |
imagery |
treatment |
Evolution (5-year follow-up) |
|
1 |
51 |
M |
14 months |
-nasal obstruction. -Epistaxis, anosmia. - Headaches. |
Left naso-ethmoïdal process With homolateral endocranien and orbital extension (T4N1M0) |
Palliative chemotherapy. (cyclophosphamide- vincristine) |
Died after the 2nd cure of chemotherapy |
|
2 |
65 |
F |
2 months |
-Nasal obstruction. -Epistaxis, anosmia. |
Localized left naso-Ethmoïdal Process (T2N0M0) |
Tumour removal, by endonasal route, followed by radiotherapy additional 50 Gy |
Complete Clinical and radiological remission |
|
3 |
50 |
M |
9 months |
-Nasal obstruction. -Rhinorhea, Epistaxis. |
Left Naso-ethmoïdal process with filling of the left maxillary sinuses and Intracranial extension. (T3N0M0) |
Tumor removal, by Endoscopic route followed by radiotherapy. |
Complete remission. |
|
4 |
63 |
M |
12 months |
-nasal obstruction. -Epistaxis -Tumefaction of the right hemiface. |
Right naso-ethmoidal process, repelling the inner wall of the right orbit, the nasal septum, the maxillary sinus and the soft jugal parts with cutaneous intrusion. (T4N1M1) |
Palliative chemotherapy. (cyclophosphamide - vincristine) |
Died 2 months after starting treatment. |
|
5 |
35 |
F |
5 months |
-nasal obstruction. -anosmia, epistaxis. -Headaches. |
process taking the Left Nasal Tassel, the sinus cavities, in contact with the medial wall of the left orbit without intracranial extension (T3N0M0) |
Surgical removal by Paralateral nasal pathway + external radiotherapy. |
Good clinical evolution |
|
6 |
40 |
F |
6 months |
-nasal obstruction. -decrease in visual acuity. (DVA) -Epistaxis. |
process of the left nasal cavity (T2N0M0) |
Surgical removal by endonasal route |
Good clinical evolution |
|
7 |
26 |
f |
6 months |
-nasal obstruction. -Epistaxis. -Exophthalmia. |
Left nasal cavity Fosse process containing calcifications + bone lysis with endoorbital extension coming to the contact of the eyeball (T3N0M0) |
Surgical removal by endonasal route followed by radiotherapy. |
Good clinical evolution |
|
8 |
40 |
H |
6 months |
-nasal obstruction. -Epistaxis -Exophthalmia -DVA |
Locally advanced right Nasal cavity process with intra- orbital and intracranial extension (T4N0M0) |
Combined tumour removal followed by complementary radiotherapy (60 Gy) |
good evolution on a current follow-up of 2 years. |
|
9 |
60 |
f |
12 months |
-Nasal obstruction. -Epistaxis |
Limited tissue process of the left FN. (T1N0M0) |
Endonasal tumor removal |
Complete remission |
|
10 |
70 |
H |
9 months |
-Nasal obstruction. -Epistaxis -rhinorrhea Exophthalmia |
Left naso ethmoidal process with orbital extension without intracranial extension. (T3N0M0) |
Combined tumor removal followed by complementary radiotherapy |
No recurrence on a current 18-month follow-up. |
|
11 |
40 |
f |
2 months |
-Nasal obstruction. -Epistaxis |
Left nasal process without locoregional extension. (T1N0M0) |
Endonasal tumor removal |
Complete remission |
|
12 |
54 |
f |
12 months |
-Nasal obstruction. -Epistaxis. -anosmia. -DVA |
Locally advanced right nasal cavity process with intra- orbital and intracranial extension |
Combined tumor removal followed by complementary radiotherapy |
Complete Clinical and radiological remission |
![Axial cut MRI T1 with gadolinium injection: large and solid process located in the nasal cavities, extended to the left maxillary sinus and invading the left orbit and anterior part of the base of the skull. [23].](https://www.jscimedcentral.com/public/assets/images/uploads/image-1724911438-1.PNG)
Figure 3: Axial cut MRI T1 with gadolinium injection: large and solid process located in the nasal cavities, extended to the left maxillary sinus and invading the left orbit and anterior part of the base of the skull. [23].
DISCUSSION
Esthesioneuroblastoma is a rare tumour that accounts for 3% of all naso-sinusal tumours [2,4]. In almost all published series, the authors report a small number of patients treated in the same institution, and the dispersion of these cases over time (often over a long period of time). It is a tumor that occurs at all ages with 2 frequency peaks, one between 11 and 20 years, the other between 50 and 60 years. It affects both sexes with a slight male predominance (Table 2).
Table 2: The authors report a small number of patients treated in the same institution, and the dispersion of these cases over time (often over a long period of time).
|
Authors |
Number of cases / Number of years |
Age/ extremes of ages |
Sex ratio (H/F) |
|
NAKAGAWA [5] |
22 cases over 8 years |
49 years (27-83) |
10/12 |
|
GAYE [6] |
12 cases over 7 years |
20 years (11-66) |
7/5 |
|
LAPIERRE [7] |
10 cases over 12 years |
56 years (32-83) |
7/3 |
|
CHAHED [8] |
3 cases over 10 years |
54 years (23-85) |
1/2 |
|
KERMANI [9] |
7 cases over 26 years |
36 years (11-63) |
2/5 |
|
Our study |
12 cases over 15 years |
48 years (26-70) |
5/7 |
Histopathogenism of esthesioneuoblastomas is little known although Volrath and Altmannsberger may have induced neurofactory tumors using nitrosamines [6,10]. The role of viruses, especially adenoviruses, is not clearly established in their carcinogenesis. However, on tumors developed spontaneously in cats, viral sequences have been found in the genome of tumor cells [10].
In a study analyzing the cytogenetic characterization of a case, numerous chromosomal aberrations were reported mainly involving chromosomes 2q, 5, 6q, 17, 19, 21q and 22, as well as Trisomy 8 [11]. Another study reported the presence of deletion of chromosomes 1p, 3p/q, 9p and 10p/q and amplifications of 17q, 17p13, 20p and 22q [12].
Ethesioneuroblastoma etiopathogenesis causes their membership in the PNET (Peripheral Neuro-Ectodermal Tumors) family to be discussed because of the frequency of T (11.22) translocation reported in Ewing’s sarcoma [13].
The clinical manifestations of Ethesioneuroblastoma can’t claim any sign of its own, especially since several symptoms can be associated, and often reflect an extensive intranasal process [10,14,15]. A well-conducted clinical examination of the ENT sphere is required to establish an early diagnosis.
CLINICAL PRESENTATION
Clinical signs are dominated by either nasosinus symptoms or evidence of the externalization of the lesion process beyond the nasosinus cavities. Rarer is the chance discovery on the systematic histological analysis of a polypectomy. Cervical lymphadenopathy is exceptional [4,16,17].
They are often late and especially not specific to a malignant process. Their banal nature and the high frequency of inflammatory or infectious pathologies of the nasosinus cavities explain that the diagnosis of these tumours is often suspected in the presence of a large lesion or accidentally on an imaging requested without back [16,18]. Faced with this banality of symptoms, certain characteristics must be taken into consideration: the one-sidedness, at least at the beginning, and the age of the manifestations that progressively lead to a worsening of the symptoms.
The esthesioneuroblastoma is characterized by high clinical variability and manifests itself in 3/4 of cases as ENT call signs [19,20]. Eye signs are associated in 11% of cases [13,19].
The CT/MRI pair allows the precise assessment of tumour extension. Indeed, MRI is crucial to clarify orbital and endocranial extension and also to differentiate between tumor mass and inflammatory retention. In advanced forms, the MRI aspect is that a dumbell-shaped tissue process centred in the upper nasal cavity and extending into the intracranial [21,22].
Based on the extension, Kadish proposed (in 1976) a 3-stage clinical classification [24]:
-Stage A: Tumor limited to the nasal cavity.
-Stage B: Tumour limited to the nasal cavity and sinuses.
-Stage C: Tumour extended beyond the nasal cavities and sinuses.
This classification was modified by Morita in 1993 [25], More recently Dulguerov [26], proposed a more accurate classification based on the TNM classification and using CT and MRI:
- T1: Tumor involving the nasal cavity and/or paranasal sinuses (excluding sphenoid), sparing the most superior ethmoidal cells.
- T2: Tumor involving the nasal cavity and/or paranasal sinuses (including the sphenoid), with/without extension to or erosion of cribiform.
- T3: Tumor extending into orbit or protruding into anterior cranial fossa, with/without dural invasion.
- T4: Tumor involving the brain.
Pathology
The histopathological aspect of esthesioneuroblastoma may be confusing with some small cell naso-sinusal tumors, especially in less differentiated forms. Immunohistochemistry is therefore of great help. In differentiated forms, the histological study shows lobules separated by conjunctivo-vascular partitions. Small to medium tumor cells have a round often nucleated nucleus and a clearly visible chromatin. The cytoplasm, which is not very abundant or moderately abundant, is poorly limited. Mitotic activity is highly variable [24,27,28]. Less frequently, the tumour is poorly differentiated, made up of diffuse layers of lymphocytoid cells, the tumour stroma is scarce and hosts a prominent capillary network. The existence of a fibrillar fund -cytoplasmic, Flexner rosettes or Homer pseudorosettes -Wright (HW) is very revealing [29]. Hyams described a 4-grade histopathological classification system that relies primarily on the level of cell differentiation, the presence of neuronal stroma, the number of mitosis and necrosis [Table 3][30].
Table 3: The Hyams histological grading system: HW rosettes, FW rosettes [30]
![The Hyams histological grading system: HW rosettes, FW rosettes [30]](https://www.jscimedcentral.com/public/assets/images/uploads/image-1724912180-1.PNG)
Treatment
Due to the rarity of esthesioneuroblastomas, the main source of assistance in making therapeutic decisions is the analysis of the results obtained by the authors who published their cases [30-32].
There is no standardized management of these tumors. The difficulty in establishing a better therapeutic strategy lies mainly in the small number of patients treated in the same institution, and in the dispersion of these cases over time (often over a long period of more than 20 years), resulting in a heterogeneity of the results [32,33].
Traditional treatment strategies are based on surgery or radiation therapy as single or combined modalities. More recently, chemotherapy has been introduced into the therapeutic arsenal of these tumours. Although there is a favourable consensus on the need for surgery, there is no agreement on the most appropriate surgical technique or on the use of complementary therapeutic methods [33,34].
For the pathway first, there is not first standard, however, any pathway first must meet two objectives: On the one hand, the possibility of controlling the entire anatomical limits of the tumor and the screened blade; On the other hand, carrying out a truly carcinological removal in monobloc, avoiding if possible Tumor fragmentation or excision by fragmentation [30]. There are basically three approaches: craniofacial, transfacial, and currently endonasal surgery is increasingly being used mainly in Kadish stages A and B [35]. The first surgical pathway is either transfacial performing a paralatero-nasal (for Kadish stages A and B), or by the upper subfrontal route if the base of the skull is reached [35,36].
In the case of an orbital extension, attitudes are extremely nuanced, but most surgical teams are currently conservative towards the eyeball; due to the lack of significant differences in survival or recurrence rates when exempted. Esthesioneuroblastoma has a high local failure rate. As a result, most institutions have adopted surgical resection followed by postoperative radiation therapy as a standard treatment approach [35].
Postoperative radiation therapy has been shown to improve local disease control. However, for early-stage disease (Kadish A) with negative resection margins, the role of postoperative radiation is still questionable and surgery alone may be sufficient [37,38]. The dose of radiation therapy used usually ranges from 55 to 65 Gy [39]. Given the complexity of the anatomy and the location and proximity of various critical structures, there was always a concern about potential complications of adjuvant radiation; However, with the advancement of radiation technologies, compliant techniques such as Intensity Modulated Radiation (IMRT) and Proton Beam Therapy have shown better results in improving local control and minimizing toxicity and complications of nearby critical structures [13,40] (Figure 4 and Figure 5).
![MRI T1 with gadolinium injection: solid intra-sinusal process (left side) with extension to the anterior cerebral fossa. [23].](https://www.jscimedcentral.com/public/assets/images/uploads/image-1724912429-1.PNG)
Figure 4: MRI T1 with gadolinium injection: solid intra-sinusal process (left side) with extension to the anterior cerebral fossa. [23].
![General appearance of the tumor. The cells are arranged according to a lobular pattern, separated by loose fibrovascular fibers. Necroses are visible in same central lobules (arrows) [29]](https://www.jscimedcentral.com/public/assets/images/uploads/image-1724912511-1.PNG)
Figure 5: General appearance of the tumor. The cells are arranged according to a lobular pattern, separated by loose fibrovascular fibers. Necroses are visible in same central lobules (arrows) [29]
The philosophy of treatment chemotherapy patients with esthesioneuroblastoma is based on the premise that these tumours share some histological features with other chemosensitive neural crest tumours (e. g. neuroblastomas, high- grade neuroendocrine carcinomas and PNETs) [41].This theory has been proven by a variety of published retrospective analyses [42,43]. While another study has suggested that perioperative chemotherapy may be harmful [44].The most commonly used schemes Cyclophosphamide (650 mg/m2) with vincristine (1. 5 mg/m2 with a maximum dose of 2 mg/m2) every 3 weeks for a total of 6 cycles [35].
Despite treatment, esthesioneuroblastoma remains a malignant tumour with a dark prognosis, since the overall survival at 5 years is of the order of 50%, and local or locoregional recurrences are very common [35] (Figure 6).
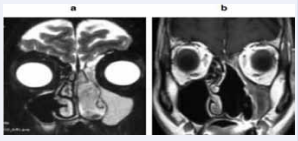
Figure 6: Coronal section of MRI. (a) pre-operative, (b) One year after treatment (Iconography of the service)
Factors that affect the Prognosis Include
? Local extension assessed according to the Kadish classification
? The histopathological grade of Hyams [30].
? Age: the prognosis would be better in a young subject after adjustment on the stage. General condition and weight loss at diagnosis would rather be related to treatment tolerance and the risk of complications [45].
? Presence of cervical lymphadenopathy at the onset of the disease:
- A meta-analysis carried out in 2008 found that the disease control was 29% in patients with lymph node invasion, compared with 64% in the opposite case [10].
- Survival at 5 years is 0% if lymphadenopathies are present, compared to 65% if not [13].
? The presence of distant metastases: indicates a very poor prognosis [13,35].
? Diffuse marking at the PS 100, a proliferation index down to Ki 67: correlated with a better prognosis [35].
CONCLUSION
Esthesioneuroblastoma is a rare malignant tumour of the olfactory placode of unknown etiology. It is characterized by clinical polymorphism, and a banality of symptoms that cause patients to reach advanced stages with significant locoregional invasion. Imaging (CTM and/or MRI) often makes it possible to evoke the diagnosis. It is an essential contribution to the evaluation of the pre-therapeutic, the determination of surgical tactics, and serves as a reference for assessing therapeutic response.
The precise diagnosis can only be made by anatomopathology. The treatment is not yet codified, but the radio association -surgical seems to give the best chance of survival. Chemotherapy is reserved for advanced stages of the disease, inoperable tumours and incurable recurrences. Despite treatment, esthesioneuroblastoma remains a malignant tumour with a dark prognosis, as the overall survival at 5 years is around 50%, and local or locoregional recurrences are very common.
References
- TanejaAK,ReisF,QueirozLS,AraújoZanardiV.Esthesioneuroblastoma. Arq Neuropsiquiatr. 2009; 67: 704-706.
- Martel J, Darrouzet V, Duclos JY, Bebear JP, Stoll D. Olfactory esthesioneuromas. Rev Laryngol Otol Rhinol. 2000; 121: 227-236.
- Berger L, Luc R. L’esthesioneuroblastome olfactif. Bull Ass Fran Cancer. 1924;13: 410-421
- Zrara I, Al Bouzidi A, Rimani M, Azendour B, Labraimi A, Ben Omar S. les esthésioneuromes (esthésioneuroblastomes) olfactifs à propos de deux cas cliniques.
- Nakagawa T, Kodama S, Kobayashi M, Sanuki T, Tanaka S, Hanai N, et al. Endoscopic endonasal management of esthesioneuroblastoma: A retrospective multicenter study. Auris Nasus Larynx. 2018; 45: 281- 285.
- Gaye PM, Mesbah L, Kanouni L, Benjaafar N, El Gueddari BK. Olfactory esthesioneuroblastoma: experience of the Rabat oncology institute and review of the literature. J Afr Cancer. 2010; 2: 36-40.
- Lapierre.A, Selmaji I, Samlali H, BrahmiT, Yossi S. Esthesioneuroblastoma: A single institution’s experience and general literature review. Cancer Radiother. 2016; 20: 783-789.
- Chahed H, Kedous S, Zainine R, Daouadi A, Mediouni A, Charfi A, et al. Esthesioneuroblastoma: diagnostic dilemma and therapeutic challenges. J Tun orl. 2014; 31.
- Kermani W, Bouattay R, Zaghouani H, Belakhder M, Ben Ali M, Abdelkafi M, et al. L’esthesioneuroblastome olfactif : à propos de 7 cas. J Tun orl. 2014; 31.
- Capelle L, Krawitz H. Esthesioneuroblastoma: A case report of diffuse subdural recurrence and review of recently published studies. J Med Imaging Radiat Oncol. 2008; 52: 85-90.
- Holland H, Koschny R, Krupp W, Meixensberger J, Bauer M, Kirsten H, et al. Comprehensive cytogenetic characterization of an esthesioneuroblastoma. Cancer Genet Cytogenet. 2007; 173: 89-96.
- Bockmühl U, You X, Pacyna-Gengelbach M, Arps H, Draf W, Petersen CGH pattern of esthesioneuroblastoma and their metastases. Brain Pathol. 2004; 14: 158-163.
- Abdelmeguid AS. Olfactory Neuroblastoma. Curr Oncol Rep. 2018; 20: 7.
- Haroussou JL, Mechinaud F, Rialland X, Milpied N, Nomballais F, Cohen JY, et al. Role of chemotherapy in the treatment of esthesioneuroblastoma in children. Apropos of 3 case reports. Ann Pediatr. 1988; 35: 383-386.
- Kriet M, Laktaoui A, Zrara S, Harmouchi N, Souhail H, Chana H, Terhzaz A. Olfactory esthesioneuroblastoma with an ophtalmological presentation: a case report. 2002; 25: 632-635.
- Simon C, Toussaint B, Coffinet L. Malignant tumors of the nasal and paranasal cavities. Oto-rhino-laryngology treatise. 1997; 20 : 405- 410.
- Guerrier B, Chantrain G, Gallaux JP Esthesioneuroblastomes olfactifs Les cahiers d’ORL, 1986, T XXI n° 9,667
- Thompson LD. Olfactory neuroblastoma. Head Neck Pathol. 2009; 3: 252-259.
- Bouziri M, Brahem D, Attia S, Ben Yahia S, Messaoud R, Khairallah M, et al. Esthesioneuroblastoma: about an observationEsthesioneuroblastoma: a case report. French Journal of Ophthalmology. 2008; 31: 21.
- Hommadi A, Akhaddar A, Fehoume K, Chakir N, Jiddane M, Boukhrissi N. Apport de l’imagerie dans l’esthesioneuroblastome a propos d’un cas. Médecine du Maghreb 2001 n°88.
- Schiro BJ, Escott EJ, McHugh JB, Carrau RL. Bone invasion by an esthesioneuroblastoma mimicking fibrous dysplasia. Eur J Radiol. 2008; 65: 69-72.
- Zhang M, Zhou L, Wang DH, Huang WT, Wang Sy. Diagnosis and management of esthesioneuroblastoma. ORL J Otorhinolaryngol Relat Spec. 2010; 72: 113-118.
- Díez-Villalba R, González-Ruiz M , Izquierdo-Vázquez C, Sanz- Fernández R, Molina-Quirós C, Colmenero-Ruiz M, et al. Ophthalmic presentation of two cases of esthesioneuroblastoma. Arch Soc Esp Oftalmol. 2008; 83: 317-320.
- Kadish S, Goodman M, Wang CC. Olfactory neuroblastoma: a clinical analysis of 17 cases. Cancer. 1976; 37: 1571-1576.
- Morita A, Ebersold MJ, Olsen KD, Foote RL, Lewis JE, Quast LM. Esthesioneuroblastoma: prognosis and management. Neurosurgery 1993; 32: 706-714.
- Dulguerov p, Allal AS, Calcaterra TC. Esthesioneuroblastoma: a meta- analysis and review. Lancet Oncol. 2001; 2: 683-690.
- Thomas J Ow, Bell D, Kupferman ME, DeMonte F, Hanna EY. Esthesioneuroblastoma. Neurosurg Clin N Am. 2013; 24: 51-65.
- Iezzoni JC, Mills SE. “Undifferentiated” small round cell tumor of the sinonasal tract: differential diagnosis update. Am J Clin Pathol. 2005; 124:110-121.
- Toader C, Stroi M, Kozma A, Arsene DE. Esthesioneuroblastoma: the complete picture – case report and review of the literature. Rom J Morphol Embryol. 2018; 59: 1211-1218.
- Hyams VJ, Batsakis JG, Michaels L Tumors of the upper aerodigestive tract and ear. 2nd series ed. Washington: Armed Forces Institute of Pathology; 1998
- Foote RL, Morita A, Ebersold MJ, O’fallon WM, Olsen KD, Lewis JE,etal. Esthesioneuroblastoma: the role of adjuvant radiation therapy. Int Journal Radiation Oncol Biol Phys. 1993; 27: 835-842.
- Bäck L, Oinas M, Pietarinen-Runtti P, Vuola J, Saat R, Ohman J, et al. The developing management of esthesioneuroblastoma: a single institution experience. Eur Arch Otorhinolaryngol. 2011; 269: 213- 221.
- Gil-Carcedo E, Gil-Carcedo LM, Vallejo LA, Campos JM. Esthesioneuroblastoma treatment. Acta Otorrinolaringol Esp. 2005; 56: 389-395.
- Turano S, Mastroianni C, Manfredi C, Viscomi C, Patitucci G, Palazzo S, et al. Advanced adult esthesioneuroblastoma successfully treated with cisplatin and etoposide alternated with doxorubicin, ifosfamide and vincristine. J Neurooncol. 2010; 98: 131-135.
- Fiani B, Quadri SA, Cathel A, Farooqui M, Ramachandran A, Siddiqi I, et al. Esthesioneuroblastoma: A Comprehensive Review of Diagnosis, Management, and Current Treatment Options. World Neurosurg. 2019; 126: 194-211.
- Ozsahin M, Gruber G, Olszyk O, Matzinger O, Zouhair A, Azria D, et al. Outcome and prognostic factors in olfactory neuroblastoma: a rare cancer network study. Int J Radiat Oncol Biol Phys. 2010; 78: 992- 997.
- Saade RE, Hanna EY, Bell D. Prognosis and biology in esthesioneuroblastoma: the emerging role of Hyams grading system. Curr Oncol Rep. 2015; 17: 1-5.
- Schwartz JS, Palmer JN, Adappa ND. Contemporary management of esthesioneuroblastoma. Curr Opin Otolaryngol Head Neck Surg. 2016; 24: 63-69.
- Suriano M, De Vincentiis M, Colli A, Benfari G, Mascelli A, Gallo A. Endoscopic treatment of esthesioneuroblastoma: a minimally invasive approach combined with radiation therapy. Otolaryngol Head Neck Surg. 2007; 136: 104-107.
- Loy AH, Reibel JF, Read PW, Thomas CY, Newman SA, Jane JA, et al. Esthesioneuroblastoma: continued follow-up of a single institution’s experience. Arch Otolaryngol Head Neck Surg. 2006; 132: 134-138.
- Cranmer LD, Chau B, Rockhill JK, Ferreira Jr M, Liao JJ. Chemotherapy in Esthesioneuroblastoma/Olfactory Neuroblastoma An Analysis of the Surveillance Epidemiology and End Results (SEER) 1973-2015 Database. Am J Clin Oncol. 2019; 43: 203-209.
- Su SY, Bell D, Ferrarotto R, Phan J, Roberts D, Kupferman ME, et al. Outcomes for olfactory neuroblastoma treated with induction chemotherapy. Head Neck. 2017; 39: 1671-1679.
- Kane AJ, Sughrue ME, Rutkowski MJ, Aranda D, Mills SA, Buencamino R, et al. Post treatment prognosis of patients with esthesioneuroblastoma. J Neurosurg. 2010; 113: 340-351.
- Alotaibi HA, Priola SM, Bernat AL, Farrash F. Esthesioneuroblastoma: summary of single-center experiences with focus on adjuvant therapy and overall survival. Cureus. 2019; 11: e4897.
- Alvarez I, Suárez C, Rodrigo JP, Nuñez F, Caminero MJ. Pronostic factors in paranasal sinus cancer. Am J Otolayngol. 1995; 16: 109- 114.








































































































































