Giant Retropharyngeal Lipoma
- 1. Department ENT - Chu Annaba, University Badji Mokhtar Annaba, Algeria
Abstract
Lipoma is a common soft tumor tissue that can develop anywhere in the body. The retropharyngeal space is a rare location for these benign tumors. Clinically it procures dysphagia, pharyngeal discomfort, snoring, or sleep apnea. Imaging (CT Scan and MRI) is necessary for diagnosis, extension, and previous surgical procedures. We report in this publication a giant lipoma of retropharyngeal space in 75 year old man diagnosed after dysphagia exploration and treated with trans cervical surgical approach.
Keywords
• Lipoma
• Retropharyngeal Space
• MR Imaging
• Cervicotomy
CITATION
Kharoubi S (2024) Giant Retropharyngeal Lipoma. Ann Otolaryngol Rhinol 11(1): 1326.
INTRODUCTION
The retropharyngeal space is an anatomical region that spans from the base of the skull to the mediastinum. This space is anterior to the prevertebral muscles and posterior to the pharynx and esophagus. In retropharyngeal space, lymph nodes, fatty tissue and small vessels are the predominant tissues. Many tumors can developed in retropharyngeal space: lipoma, schwannoma, retropharyngeal abscess, branchial cysts, squamous carcinoma, liposarcoma, synovial sarcoma, metastatic adenopathy and lymphomas (Table 1).
Table 1: Summary of retropharyngeal tumors colliged by the author between 2000 and 2023. F: Female; M: Male
|
CASE |
YEAR |
AGE |
GENDER |
PATHOLOGY |
TREATMENT |
|
1 |
2000 |
58 |
M |
SQUAMOUS CARCINOIMA |
TRANS ORAL |
|
2 |
2005 |
77 |
M |
CHORDOMA |
TRANS CERVICAL |
|
3 |
2005 |
12 |
F |
ABSCESS |
TRANS ORAL |
|
4 |
2007 |
52 |
M |
TUBERCULOSIS |
TRANS ORAL |
|
5 |
2008 |
10 |
F |
ABSCESS |
TRANS ORAL |
|
6 |
2020 |
12 |
M |
LYMPHOMA (NHL-B) |
TRANS ORAL |
|
7 |
2023 |
75 |
M |
LIPOMA |
TRANS CERVICAL |
|
8 |
2023 |
66 |
F |
CHORDOMA |
TRANS ORAL |
Lipomas in the head and neck are more uncommon accounting for 25% of all lipomas and 1% of them in retropharyngeal space [1]. The extending space, slow growing and deep lesion may go undiagnosed and the symptomatology associate dysphagia, dyspnoea and snoring. Imaging MRI (Magnetic Resonance Imaging) facilitate size, extension and nature of the lesion. The management was surgical.
CASE PRESENTATION
75 year old man, presented to our ENT department with progressive dysphagia and dysphonia. He reports since three months dyspnea after efforts with recent aggravation. He reported also, snoring and sometimes sleeping apnea. The clinical exam showed a swallowing neck predominates on the right side homogenous, without pain and farm after palpation. Flexible nasal endoscopy noted a diminution of the mobility of the right vocal plica. A cervical ultrasound exam noted a homogenized and enlarged cervical mass (Figure 1,2).
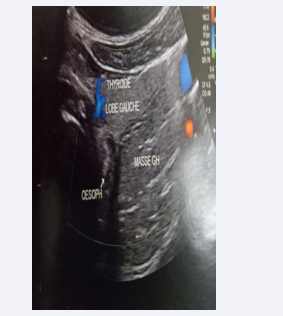
Figure 1: Ultrasonography - Left Cervical part: homogenic mass compressed left thyroid lobe laterally to esophagus.
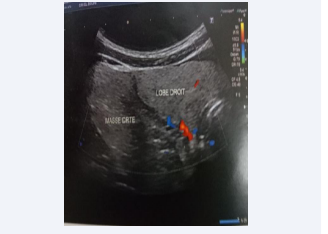
Figure 2: Ultrasonography- Right Cervical part: homogenic mass compressed right thyroid lobe.
A CT scan found the largest tumor homogenous occupied retropharyngeal in lateral cervical space, suggesting lipoma. MRI confirmed the diagnosis of retropharyngeal giant lipoma with cervical (right) extension. There was no invasion to the neighboring structures (Figures 3-6).
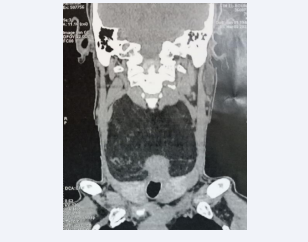
Figure 3: Coronal CT image showing large fat density mass occupied cervical space compressing trachea
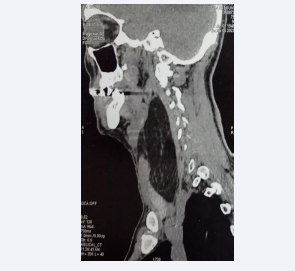
Figure 4: Sagittal reformatted CT image showing fat density mass in the retropharyngeal space.
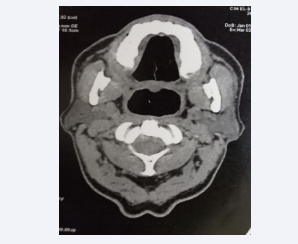
Figure 5: Axial CT Scan showing fat density mass in retropharyngeal space
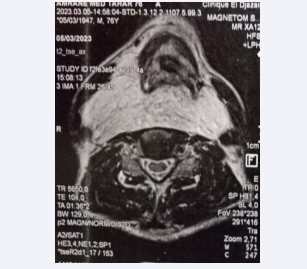
Figure 6: Axial RM image showing largest mass (fat) hyper intense signal on fat satured T2WI.
A right cervicotomy exposed the lesion and we removed a giant lipoma (30x20cm) after separating neurovascular structures (Figure 7). A histopathologic exam confirmed benign lipoma (fibrolipoma) and the fellow up was simple.
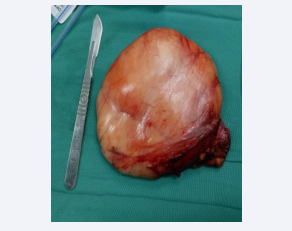
Figure 7: Surgical specimen well circumscribed with thin fibrous capsule.
DISCUSSION
Lipoma is the most common benign mesenchymal tumor and can virtually develop anywhere in the body [2]. The mean age of patients was 49.9 years, with a range from 2 years to 81 years as common in men. It’s also described in child (snoring) [3]. The can sporadically occur as part of syndromic lipomatosis such as Madelung’s disease or Launois-Bensaude syndrom [4].
Between 2000 and 2020, Alnami reported 27 cases of retropharyngeal lipomas [5]. Our review of the literature has found four supplementary cases.
The clinical presentations of patients with retropharyngeal lipomas varied widely. The major symptom is a progressive dysphagia and unintentional weight loss. We can also found, snoring, rhinolalia, pharyngeal discomfort, and sleep apnea, fortunately discovered after imaging [6,7].
Lipomas appear as soft variably echogenic masses, commonly encountered on ultrasound, without or minimal color Doppler flow. Furthermore, heterogeneous echotexture, more than minimal color Doppler flow, or large size is suspicious for liposarcoma [8]. On CT, the retropharyngeal lipoma appears as a well-circumscribed non-enhancing lesion with homogeneous fat attenuation. Ehlers report one case in 66 year-old-female diagnosed after cone beam computed tomography (CBCT) in pre implant dental cheek [1].
On MR images, fat has typical signal intensity on T1 weighted images, they tend to have high signal intensity that decreases with progressive T2 weighting. The relationship between the lipoma and the prevertebral muscles is noted as well as the possibility of a liposarcoma. Fat tissue ranging between - 50 to 150 Hounsfield units [8]. The lesion may contain thin septa.
Fine-needle aspiration cytology (FNAC) can help with the diagnosis, but definitive diagnosis requires on histological confirmation after surgical excision.
While the transoral approach (classically or by transoral robotic surgery) is often preferred since it has lower morbidity, we performed the transcervical approach considering the giant size of retropharyngeal lipoma [6]. Varghese removed a 12 X 11,7 cm retropharyngeal lipoma by trans oral approach [9].
Bowers choose anteriortrans cervical procedure after larynx rotated medially to acces the anterior border of the spine and removed an osteolipoma of retropharyngeal space [10].
Lipoma may have different histologic subtypes, including angiolipoma, fibrolipoma, chondrolipoma, myxoid lipoma, pleiomorphic lipoma, spindle cell lipoma and osteolipoma [10,11].
The principal differential diagnosis is the well differentiated liposarcomamay be suspected by imaging (Doppler color, relationship with prevertebral muscles in RM images, fine needle aspiration cytology) but essentially through histopathologic exam (immunohistochemistry) [12].
There is no evidence of malignant transformation or recurrence after complete resection of a retropharyngeal lipoma [2].
CONCLUSION
Retropharyngeal lipomas are rarely reported as an etiology of dysphagia in adults. Clinical exam can shows an enlarged tumor of retropharyngeal (oropharyngeal exam) or parapharyngeal space (cervical exam). CT and imaging MR are necessary to recognize lipoma, extension cheek and ideal surgical procedure (transoral or trans cervical).
REFERENCES
2. Barnes L. Tumors and tumor like lesions of the head and neck. Surgical pathology of the head and neck New York. Marcel Decker Inc. 1985; 747-58.







































































































































