Lateral Canal Benign Paroxysmal Positional Vertigo: A Review of its assessment and Treatment Options
- 1. Department of Audiology and Phoniatrics, G. Rummo Hospital Benevento, Italy
ABSTRACT
Benign paroxysmal positional vertigo (BPPV) is the most common vestibular syndrome. It is characterized by short lasting spelling of vertigo when patient change his/her head position in the space. The putative pathogenesis is the dislodgement of otoliths from the utricular macula to semicircular canals. The most frequent form is posterior canal BPPV, whereas lateral canal BPPV is reported in about 20% of cases. Various forms of lateral canal BPPV are reported: geotropic variant, apogeotrophic variant and, more recently, a Direction-fixed nystagmus variant, which is the rarest form. Mechanisms other than canalar lithiasis could be involved in the pathogenesis of lateral canal BPPV, namely situations of “heavy cupula’’ and “light cupula”. Liberatory therapy is very effective and the shift from an apogeotrophic form to a geotropic form is considered useful for a better outcome. Aim of the paper is to present a review of current pathophysiological hypothesis about lateral canal BPPV, its assessment and therapeutic options
KEYWORDS
BPPV, Lateral canal, Canalolithiasis, Cupulolithiasis, Liberatory therapy, Heavy cupula, Light cupula
CITATION
Califano L, Salafia F, Melillo MG, Mazzone S (2015) Lateral Canal Benign Paroxysmal Positional Vertigo: A Review of its assessment and Treatment Options. Ann Otolaryngol Rhinol 2(6): 1046.
INTRODUCTION
Benign Paroxysmal positional vertigo (BPPV) is the most frequent vertiginous syndrome [1,2]. The posterior canal (PC) is mostly frequently involved (75-85%), lateral canal (LC) is involved in 15-20%, whereas the rarest condition is anterior canalolithiasis (AC) (< 5%). BPPV is characterized by brief recurrent spells of vertigo when the patient changes his/ her position; during an acute spell of vertigo, nystagmus is paroxysmal, torsional and vertical in PC-BPPV and AC-BPPV, paroxysmal and horizontal in LC-BPPV. BPPV is usually caused by free-floating otoconia dislodged from the utricle in the semicircular canals (canalolithiasis). Less frequently, otoliths adhere to a semicircular canal cupula, rendering it heavier than the surrounding endolymph (cupulolithiasis). Both conditions are able to change the firing rate of the vestibular nerve causing oculomotor responses through neural pathways; each canal has excitatory connections to extraocular muscles, so that eye movements happen in the same plane of the stimulated canal.
BPPV is a lot more frequent in adulthood, it is often idiopathic and is frequently caused by head injuries; association with migraine and autoimmune disease is reported [1,2]. Both the frequency of BPPV observation and the availability of higheffective liberatory maneuvers caused a lot of specialistic reports in the last 25 years.
In 1985, the lateral canal BPPV was described, individually, by Cipparrone and Pagnini [3] and McClure [4]. In lateral canal BPPV nystagmus is horizontal and usually paroxysmal, evoked trough a patient’s head rotation in the yaw plane while supine (Head yaw Test-Pagnini-Mc Clure Test). Based on the nystagmus direction, lateral canal BPPV was distinguished in geotropic and apogeotropic forms [5,6]: in the geotropic form, nystagmus fast phases beat toward the under most ear, both on the affected side and on the healthy side; in the apogeotropic form nystagmus fast phases beat toward the uppermost ear both on the affected side and on the healthy side. In the geotropic form, the affected side is where nystagmus is the strongest; instead, in apogeotropic lateral canal BPPV, the affected side is where the nystagmus is the weakest. When the affected side is lowermost, a nystagmus second phase, opposite in direction to the first phase, is sometimes observed, more frequently in geotropic forms.
Recently, we described a rare form, the “direction-fixed” nystagmus lateral canal BPPV, [7] in which nystagmus always beats toward the same side, either when the affected ear is uppermost or when it is lowermost, with a greater intensity on the side where it is apogeotropic, which is often the affected side.
In lateral canal BPPV, the positioning nystagmus respects Ewald’s laws: it is horizontal, like the involved canal plane (Ewald’s first law) and its intensity is greater in the position that gives an ampullopetal excitatory stimulation than in the contra lateral position which provokes an ampullofugal inhibitory stimulation (Ewald’s second law) (Figure 1).

Figure 1: Left lateral canal geotropic BPPV, positioning on the left side: otoliths are in the non-ampullary arm.
This happens on the affected side in the geotropic forms, admitting that otoliths are positioned in the non-ampullary tract of the lateral canal (Figure 2),

Figure 2: Left lateral canal apogeotropic BPPV, positioning on the left side: otoliths are in the ampullary arm or on the cupula.
and on the healthy side in the apogeotropic forms, admitting that otoliths are located or in the ampullary arm of the lateral canal (canalolithiasis) or on the lateral canal cupula (cupulolithiasis) (Figure 3).

Figure 3: Left Direction fixed nystagmus lateral canal BPPV, positioning on the left side.
In the Direction fixed nystagmus lateral canal BPPV otoconial debris could be present in multiple canalar parts, either in the ampullary arm and in non ampullary arm (Figure 4).

Figure 4: Mechanism of leaning nystagmus in sitting position.
Nystagmus is the algebraic sum resulting from ampullophugal and ampullopetal endolymphatic flow. Direction fixed lateral canal BPPV is usually converted either through repeated Head Pitching maneuvers or through repeated latero-rotations of patient’s head in the supine position in a typical geotropic or apogeotropic form.
In lateral canalolithiasis Nystagmus often persists more than one minute, more than three minutes in lateral cupulolithiasis. Some horizontal non-paroxysmal nystagmus forms have been described [8-12], in the “heavy cupula” condition, which provokes an apogeotropic persistent nystagmus and in the “light cupula” condition, which provokes a geotropic persistent nystagmus.
Horizontal paroxysmal bidirectional positioning nystagmus represents the main diagnostic sign of lateral canal BPPV; some authors described other signs- secondary signs- [13], that can be observed either in sitting position- pseudo-spontaneous nystagmus [14], Bowing and Leaning nystagmus [15], Null point in the pitch plane [13,14], Head Shaking induced nystagmus [13] or in the supine position- Lying down nystagmus [16], Null point in the horizontal plane [17], second phase of the paroxysmal nystagmus [13]. Secondary signs are useful to identify the affected side, especially when the nystagmus intensity differences are not clear at Pagnini-Mc Clure test [13].
Pseudo-spontaneous nystagmus, leaning nystagmus and lying-down nystagmus beat towards the healthy side in the geotropic form, and toward the affected side in the apogeotropic form; bowing nystagmus beats towards the healthy side in the apogeotropic form, and toward the affected side in the geotropic form. Their pathophysiology is well explained by the canalolithiasis hypothesis: the channel works as an inclined plane on which otoliths slide in various direction, depending on the spatial plane canal position, as reported by AsprellaLibonati in a unitary theory about free-floating otoliths in BPPV[18]. In the geotropic form, in leaning and lying down positions (Figure 5)

Figure 5: Mechanism of lying down nystagmus.
otoliths slide towards the non-ampullary tract of the canal, causing a nystagmus beating toward the healthy side, due to an ampullophugal inhibitory endolymphatic flow. In the apogeotropic form, in the same positions, the opposite occurs: leaning nystagmus and lying down nystagmus beat toward the affected side, due to an ampullopetal excitatory endolymphatic flow. The opposite happens for the bowing nystagmus (Figure 6):

Figure 6: Mechanism of bowing nystagmus in sitting position.
nystagmus beats toward the affected side in leaning and lying down positions, due to an ampullopetal excitatory endolymphatic flow, toward the healthy side in the bowing position, due to an ampullophugal inhibitory endolymphatic flow. Null point represents the position of the canal in which nystagmus disappears, either in the pitching plane or in the yaw plane; null points are determined by the position of the lateral canal in which the axis of the cupula is vertically aligned to the gravitational axis [11,18].
Mechanisms other than canalolithiasis: Endolymph/ cupula modified density ratio
Heavy cupulaCupulolithiasis is the condition most frequently associated with a heavy cupula- otoliths coated on the lateral canal cupula- but, other type of material may cause it, such as blood or macromolecular aggregates. When the patient’s head is carried from the supine position to the affected side, the cupula, due to gravitational vectors, will deflect in the ampullofugal sense, and a long lasting apogeotropic nystagmus is observed; when the “heavy cupula” is positioned uppermost, it will deflect in ampullopetal sense, causing an apogeotropic nystagmus, which is greater than the one observed on the affected side.
Light cupula It is the pathophysiological condition opposed to the “heavy cupula”, similar to post alcoholic nystagmus. Endolymph is heavier than the cupula, causing an ampullopetal endolymphatic current. Therefore, nystagmus is geotropic, persistent, more intense on the affected side, with duration of several minutes. Either “light” bodies on the cupula or the presence of endolymphatic heavy bodies could explain this condition. An about 20° mild head rotation toward the affected side results in an alignment of the cupula gravitational axis and, therefore, the nystagmus disappearance (null point on the yaw plane) [12]. Marginal stria blood flow alterations [19] may cause modification of the endolymphatic homoeostasis, provoking changes in endolymph density, or making it heavier than the cupula (light cupula), or making it lighter than the cupula (heavy cupula). The presence either of inflammatory endolymphatic cells, demonstrated in experimental models [20,21] or of watersoluble macromolecules concentration changes in endolymph [22] may result in endolymph density changes, responsible for situations either of “light cupula” or of “heavy cupula”.
Conversion from apogeotrophic lateral canal BPPV to geotropic lateral canal BPPV
The shift from from an apogeotropic form to a geotropic form improves the therapeutic outcome [16], because otoliths move from the ampullary arm to the non ampullary arm, which is closer to the utricular exit of the canal, i.e. the road that otoliths follow to exit from the canal during any therapeutic maneuver.
The shift may be achieved trough several different maneuvers: Head Pitching maneuver (HPM) in sitting position [23] (Figure 7);

Figure 7: Possible mechanism of the conversion from apogeotropic to geotropic canalolithiasis through Head Pitching Maneuver.
side to side rotations in the supine position [16]; mastoid oscillation [24]; Head Shaking in the supine position [25]; Gufoni liberatory maneuver towards the affected side [26]; Forced prolonged position on the affected side (FPP) [27].
Conversion trough HPM, side to side rotation or the first step of the Gufoni maneuver towards the affected side is due to the movement of otoliths away from the cupula, toward the non ampullary arm, by inertial forces; instead, in FPP, the transformation is based on a progressive gravitational movement of otholits toward the non ampullary arm. The shift from an apogeotropic form to a geotropic form occurs in ampullary arm canalolithiasis and not in cases of cupulolithiasis or heavy cupula, because in these cases otoliths are strictly adherent to the ampullar cupula. The synopsis of a possible classification of lateral canal BPPV based on the position of otoliths in different tracts of the lateral canal is reported in Table 1.
Table 1: Clinical forms of lateral canal BPPV.
| Location of otoliths | Clinical form | Frequency | |
| Lateral canal | Non-ampullary arm | Geotropic lateral canal BPPV | High |
| Lateral canal | Ampullary arm | Apogeotropic lateral canal BPPV | Middle |
| Lateral canal | Cupula | Apogeotropic lateral canal BPPV (lateral cupulolithiasis) | Middle |
| Lateral canal | More tracts | "Direction-fixed Nystagmus" lateral canal BPPV | Low |
The treatment of lateral canal BPPV
Some evidences exist about the efficacy of liberatory maneuvers for lateral canal BPPV. Mandalà et al [26] reported a 1B-Level of evidence for Gufoni maneuver [27] in 72 patients with unilateral LC-BPPV, recruited for a double-blind randomized trial in a multicentric study; Kim [28] reported a Class 1 evidence that barbecue rotation maneuver and Gufoni maneuver are effective in treating geotropic lateral canal BPPV; Kim [29] in a randomized clinical trial reported evidence for the efficacy of the Gufoni maneuver in treating apogeotropic lateral canal BPPV; a systematic review by van den Broek [30] showed that the Gufoni maneuver was more effective than a sham maneuver or vestibulo-suppressants in treating lateral canal BPPV. Chiou [31] reported a high rate effectiveness of the Forced Prolonged Position [32] in treating both geotropic and apogeotropic lateral canal BPPV; Chu [33] considered the Forced Prolonged Position an excellent treatment for geotropic lateral canal BPPV. Dataset of these reports showed similar rates of effectiveness for every of the reported treatments.
Forced Prolonged Position [32]
To treat geotropic lateral canal BPPV, the patient lies on the healthy side at least for 12 hours. The prolonged position allows otoliths to leave the affected canal, moving slowly toward the utricle. In the apogeotropic variant, the first step needs a prolonged position on the affected side to cause the displacement of otoliths from the ampullary arm to the non ampullary arm of the lateral canal. After the conversion in the geotropic form, the patient will lie on the healthy side for about other 12 hours, to complete the otoliths movement toward the utricle.
Gufoni maneuver [27] (Figure 8)

Figure 8: Gufoni Maneuver for right geotropic lateral canal BPPV (or for left apogeotropic lateral canal BPPV).
In the geotropic variant, the patient is quickly brought from the sitting position to the lateral position on the healthy side and then his/her head is turned 45° downward. After 2-3 minutes the patient returns to the sitting position. In the apogeotropic variant, the same maneuver is performed toward the affected side; the conversion in a geotropic form is attended, but sometimes a direct resolution of the disease is obtained. In the variant proposed by Ciniglio Appiani [34] for the apogeotropic form, the patient’s head is turned 45° upward. The Gufoni maneuver could act through the inertial detachment of otoliths caused by the brisk deceleration of the head and their migration toward the utricle or the canal.
Barbecue rotation maneuvers (35-37) [Figure 9]
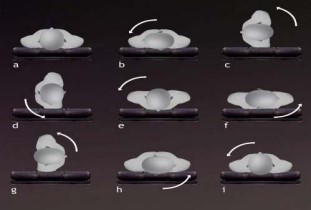
Figure 9: Barbecue rotation maneuver for right lateral canal BPPV.
In the supine position, patient’s head and body are quickly rotated by 90° steps from the affected side to the healthy side both in geotropic and in apogeotropic forms for a total of 180° , 270° , or 360° . The patient is then brought to the sitting position. Asprella Libonati [38] proposed a variant of the maneuver: the patient is brought from the sitting to the supine position and his/her head is turned 90° toward the healthy side; after 30 seconds the patient returns to the sitting position and his/her head is brought in line with the body; the maneuver is repeated five times
What in the next future? The main problems of BPPV are related to the understanding of metabolic disorders that could lead to the abnormal release of otoliths from utricular macula and their dislodgement in the semicircular canals. Metabolic problems due to alterations of the mechanisms of the production of the endolymph could cause changes either of the endolymph/ cupula weight ratio or of the reabsorbtion of otoliths, either in utriculus or in the semicircular canals. Morphological abnormalities of the canal could cause the entrapping of otoliths in several parts of the canal, accounting, for example, for the rare form of Direction-fixed nystagmus lateral canal BPPV. It is also possible to think that alterations in the central control system can lower the threshold of excitability of semicircular canals. Otolith metabolism, alteration of the morphology of semicircular canal,alterations of the central inhibition mechanism, in our opinion, is the etiopathogenetic aspects that future researchers should analyse in solving actual BPPV problems.








































































































































