Multiple Space Infection of the Neck Due to Klebsiella pneumoniae Infection, Recovery after Surgical Debridement-A Case Report and Literature Review
- 1. Department of Stomatology, The Affiliated Hospital of Qingdao University, Shandong Province, Qingdao 266000, China
- 2. School of Stomatology, Qingdao University, Shandong Province, Qingdao 266000, China
- #. Author contributed equally to the article
Abstract
Gas gangrene is a rapidly progressing and potentially fatal infection commonly found in the extremities. Head and neck gangrene is a very rare disease, and klebsiella pneumoniae infection caused by a neck abscess formed by non-clostridium gas is unusual. We report a rare case of klebsiella pneumoniae infection resulting in deep gas gangrene of the neck leading to septic shock and multiple organ failure, which recovered after surgical debridement of the neck. This is a potentially fatal disease that requires emergency drainage due to its high mortality rate.
Keywords
• Klebsiella pneumonia
• Multiple organ failure
• Interstitial infection
Citation
Li D, Wei Y, Wang S, Wang L (2025) Multiple Space Infection of the Neck Due to Klebsiella pneumoniae Infection, Recovery after Surgical Debridement-A Case Report and Literature Review. Ann Otolaryngol Rhinol 12(2): 1355.
INTRODUCTION
Gas gangrene is a very rare and life-threatening necrotic disease in which soft tissue infections progress rapidly and most commonly occur in the extremities. Gas gangrene occurs very rarely in the head and neck and is usually seen in unusual cases, with a neck abscess caused by klebsiella pneumoniae. Klebsiella pneumoniae is a kind of gram-negative bacillus. Its virulence factors include capsular polysaccharide, pili, outer lipopolysaccharide, bacterial protein and ferrifera, etc [1,2]. It is widely present in the normal flora of the mouth, skin and intestine and has become an important pathogen, with pneumonia being the most common infection outside hospitals. Gas gangrene is a rare disease that can lead to sepsis and septic shock after the bacteria enter the bloodstream [3]. This is a report of neck space infection in a diabetic patient. The patient had left submaxillary and parapharyngeal abscess with gangrene caused by klebsiella pneumoniae infection, sepsis with high fever, and recovered after neck debridement.
CASE REPORT
The patient was a 69-year-old male. The patient had left neck swelling, local redness, tension, pain, high fever, and a maximum body temperature of 41? before 1 week without apparent reason. The swelling of the posterior neck continues to increase, the swelling of the submandibular region, and the contour of the lower margin of the mandible disappears, affecting eating and pronunciation. Ultrasound-guided puncture was performed in the outpatient department, with little air extraction and no obvious fluid outflow. At the time of reporting, his blood pressure was 120/72mmHg, his heart rate was 68 beats per minute, his body temperature was 40°C, and his breathing rate was 17 beats per minute. Oral examination showed no diseased teeth and infection. In addition, the patient had diabetes, fasting blood glucose of 16.01mmol/L, and urinary ketone bodies (+++). The patient presented with severe sepsis resulting in multiple organ dysfunction syndrome, resulting in multiple abnormalities in laboratory results (Table 1). The Acute Physiological and Chronic Health Assessment (APACHE) II score was 41.
Table 1: Laboratory findings.
|
Blood Analysis |
Blood Biochemistry |
Blood Gas |
|||
|
WBC counts |
12.7 109/L |
Creatinine |
62.4 umol/L |
pH |
7.22 |
|
Neutrophil |
86.7 % |
Total bilirubin |
16.4 umol/L |
PCO2 |
25.00 mmHg |
|
Platelet count |
254 109/L |
AST |
367 U/L |
PO2 |
117.00 mmHg |
|
Hematocrit |
35 % |
ALT |
123 U/L |
HCO3 |
12.60 mmol/L |
|
Lymphocyte ratio |
8.6 % |
Albumin |
37.7 g/L |
|
|
|
aPTT |
54.4 seconds |
Glucose |
16.01mmol/L |
|
|
|
|
|
HbA1C |
9.8 % |
|
|
An emergency computed tomography scan of the neck revealed a liquefaction cavity and a large amount of gas in multiple Spaces of the left submaxilla and neck (Figure 1 A). Neck exploratory drainage was performed 3 hours after arrival at the hospital. Necrotic tissue and pus were removed, and a large number of bubbles were seen (Figure 1 B). Both aerobic and anaerobic culture of pus showed klebsiella pneumoniae. Meropenem and albumin were given intravenously and extended infusion was given. Intravenous infusion of meropenem 1g/12h was continued for 7 consecutive days, and the surgical wound was alternately washed with normal saline and diluted iodophor solution every day. The infection resolved after 2 weeks. The patient’s fasting blood glucose was controlled at 5.6mmol/L, urine ketone body (+), and body temperature was normal.
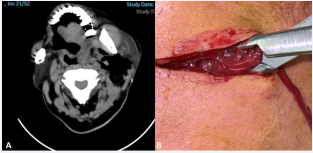
Figure 1 (A) An emergency computed tomography scan of the neck revealed a liquefaction cavity and a large amount of gas in multiple Spaces of the left submaxilla and neck. (B) Necrotic tissue and pus were removed, and a large number of bubbles were seen.
DISCUSSION
80-95% of gas gangrene is caused by Clostridium perfringens. However, other Clostridial species and other microbes such as E. coli have also been isolated. In the cases of recent years, pus culture showed klebsiella pneumoniae, which is a very rare gas-forming abscess [4]. Klebsiella pneumoniae is a gram-negative, nonmotile, encapsulated opportunistic pathogen that generally colonises human mucous membranes, including the nasopharynx and gastrointestinal tract and is ubiquitously found in soils and the healthcare environment such as on the surfaces of medical devices. K. pneumoniae has been prioritized as one of the top three pathogens of international concern in 2017 by the World Health Organization being a clinically important pathogen causing various infections such as urinary tract infections, respiratory infections, bacteremia, and pneumonia etc.
Gas gangrene caused by this bacterium is extremely rare and only a few reports have been made to date [4]. We report here a man with diabetes mellitus who was diagnosed with gas gangrene of the neck, both aerobic and anaerobic culture of pus showed klebsiella pneumoniae. Cervical necrotizing fasciitis tends to involve deep tissue and spread caudally to the chest and mediastinum resulting in catastrophic complications. Gas gangrene progresses more rapidly, leading to severe morbidity and high mortality. There is a positive statistical correlation with significance (p<0.5) between disease severity and patient with underlying disease such as diabetes mellitus, cancer and uraemia4.
Our patient had diabetes, fasting blood glucose of 16.01mmol/L, and urinary ketone bodies (+++). Neck exploratory drainage was performed 3 hours after arrival at the hospital. Gas gangrene of neck spaces occurs most frequently as a result of acute pharyngolaryngeal inflammation, followed by odontogenic infections, unknown etiology Uncommon. Respiratory and odontogenic infections were not detected in this case and there were no other obvious abnormalities. Whereas the patient presented with sepsis on admission. This could be an infection of unknown etiology colonising the neck through the bloodstream. Bacterial cultures often show polymicrobial organisms, with Klebsiella often being the culprit [5]. In 1983, K. pneumoniae was first reported to produce extendedspectrum beta-lactamases [5].
In addition, studies in recent years have found that Carbapenem-Resistant K. Pneumoniae (CRKP) started to emerge, and an increase in CRKP isolates from 29% in 2008 to 57% in 2016. Nowadays, tigecycline and colistin are used as the ultimate drug options in the treatment of multidrug-resistant K. pneumoniae infections. However, an Italian report showed a 43% colistin resistance from carbapenem-resistant isolates collected5. There is a possible evolution of colistin resistance in a setting with high klebsiella pneumoniae carbapenemase-producing klebsiella pneumoniae. Our patient was given meropenem 1g/12h intravenously for 7 consecutive days, and on the third day, blood culture showed klebsiella pneumoniae negative.
It is evident that this case is not carbapenem-resistant K. pneumoniae infection. In conclusion, we report a case of klebsiella pneumoniae infection of unknown origin resulting in gas gangrene of the neck. Timely execution of surgical neck debridement and broad-spectrum antibiotic therapy. This is a pathogenic disease. Predisposing medical conditions include old age and an immunocompromised state such as diabetes mellitus and malnutrition results in increased tendency to develop necrotizing fasciitis. Early diagnosis, timely incision and drainage and aggressive debridement are essential.
DECLARATIONS SECTION
Human Ethics
Informed consent was obtained from each patient for this retrospective study.
Consent for publication
All the authors have consented to publication.
Competing interests
All authors have no direct conflict of interest.
FUNDING
Funded by National Natural Science Foundation of China “Study on the mechanism of EFNA3 induced oral squamous cell carcinoma regulated by KMT2D through H3K4me1/H3K27ac” (82203418)
AUTHORS’ CONTRIBUTIONS
Li DP: Contributed to design, acquisition, analysis,and interpretation, drafted manuscript, critically revised manuscript.
Wei YB: Contributed to design, acquisition, and interpretation, drafted manuscript, critically revised manuscript, gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Wang SY: Contributed to design, acquisition, and interpretation, drafted manuscript, critically revised manuscript, gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Wang L: Contributed to design, acquisition, and interpretation, drafted manuscript, critically revised manuscript, gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
All authors gave their final approval and agree to be accountable for all aspects of the work.
References
- Nguyen D, Yaacob Y, Hamid H, Muda S. Necrotizing Fasciitis on the Right Side of the Neck with Internal Jugular Vein Thrombophlebitis and Septic Emboli: A Case of Lemierre’s-Like Syndrome. Malays J Med Sci. 2013; 20: 70-78.
- Gamoh S, Tsuji K, Maruyama H, Hamada H, Akiyama H, Toda I, et al. Gas gangrene in the deep spaces of the head and neck visualized on computed tomography images. Oral Radiol. 2018; 34: 83-87.
- Kiddee W, Preechawai P, Hirunpat S. Bilateral septic cavernous sinus thrombosis following the masticator and parapharyngeal space infection from the odontogenic origin: a case report. J Med Assoc Thai. 2010; 93: 1107-1111.
- Ah YM, Kim AJ, Lee JY. Colistin resistance in Klebsiella pneumoniae. Int J Antimicrob Agents. 2014; 44: 8-15.
- Dixit A, Kumar N, Kumar S, Trigun V. Antimicrobial Resistance: Progress in the Decade since Emergence of New Delhi Metallo-β- Lactamase in India. Indian J Community Med. 2019; 44: 4-8.








































































































































