The Use of Autologous Fascia Lata Graft Aided with Pedicled Muscle Flap in the Repair of Pharyngeal Tears
- 1. Department of Otorhinolaryngology, Ain Shams University, Egypt
ABSTRACT
Introduction: Management of pharyngo-esophageal tears is challenging as it can end in mediastinitis and/or carotid blow out. Pharyngo-esophageal tears accompanied by suppuration or other neck’s vital structures injuries are more complicated.
Patients and Methods: This study addressed the use of non-vascularized autologous fascia lata graft in addition to a pedicled sternomastoid flap as a second layer in the repair of wide, primary irreparable pharyngeal tears. This was done to four patients with pharyngeal tears at Ain Shams University Hospitals, Cairo, Egypt. Pre and post-operative laryngeal examination, CT scan neck with contrast swallow were done.
Results: All patients showed complete closure of the pharyngeal tear. The harvesting of the grafts produced neither functional deficits nor complications at the donor site.
Discussion: The procedure was found to be effective with complete sealing of the tear as proved clinically and radiologically.
KEYWORDS
Pharyngeal tear-fascia lata-gunshots
CITATION
Tiba M, Hasaballah M, Askoura A, Kassamy H (2015) The Use of Autologous Fascia Lata Graft Aided with Pedicled Muscle Flap in the Repair of Pharyngeal Tears. Ann Otolaryngol Rhinol 2(5): 1037.
INTRODUCTION
The fascia lata is the deep fascia of the thigh – a veritable stocking forming an ectoskeleton for its muscles. It is a trilaminar fibrous tissue sheath that envelops the muscle groups-of the thigh. It gives rise to three thickened intermuscular septa that define the thigh’s compartments and through which it is anchored to the femur. It is thicker laterally than medially (where it is more exposed), and the thickening is called the iliotibial (IT) tract or band [1]. Fascia lata proved to be excellent, strong, pliable, and easily sutured to native tissues. It is homologous tissue with no risk of foreign body reaction and a very low risk of infection. The fibrous sheet-like nature of fascia permits it to be cut and shaped as required in any type of reconstructive procedure [2]. Because of the relative a cellular nature and the low nutritional requirements of fascia, fresh autogenous fascia lata is a more desirable material because there is minimal to no tissue reaction or rejection and it maintains its original tensile strength. Thus it is widely used in different fields of reconstructive surgeries [3]. It is also used in rhinoplasties as a reliable, simple method for camouflaging any postoperative dorsal irregularities [4] or combined with crushed cartilage for dorsal augmentation and contouring [5]. It is also used in repair of wide septal perforations [6]. Early diagnosis of pharyngeal tears is mandatory and crucial in the management steps of gunshot injuries to the neck. Once suspected, endoscopy or esophagography should be used to confirm the presence of a pharyngeal tear. Primary repair has the advantages of faster recovery and shorter inpatient care duration, and reducing the risk of salivary leakage in the neck. For patients with recognized tears, primary repair with tissue reinforcement, followed by short-term esophageal rest via NGT placement and intravenous antibiotic therapy is preferable [7].
PATIENTS AND METHODS
The current study that was held in Ain Shams University hospitals in 2013 and 2014discussedthe use of autologous fascia lata graft (AFLG) aided with pedicled muscle flap in the repair of pharyngeal tears. This study included four patients; three adult male patients presented to the emergency room with history of gunshot in the neck, neck swelling, stridor, absolute dysphagia, hematemesis, and shock. They were subjected to ant shock measures, nasogastric tube (NGT) insertion, CT scan neck without contrast (Figure 1),
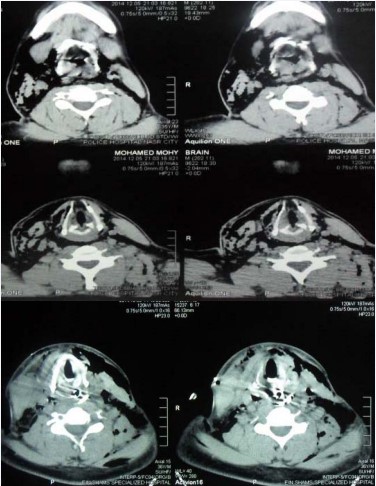
Figure 1: CT scan neck axial cuts showing multiple levels of surgical emphysema, edema of the entire laryngeal lumen and completed separation of the larynx and pharynx from the prevertebral muscles and fascia by air.
gastrographin swallow (Figure 2)
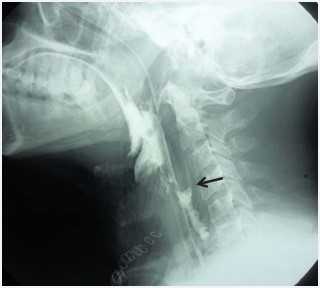
Figure 2: Gastrographin swallow. Showing loss of cervical lordosis denoting neck muscles spasm, widening of the prevertebral space due to edema and surgical emphysema. Ba leak into the retropharyngeal space (arrow) is noted at the level of upper border of C4.
and CT scan neck with gastrographin swallow (Figure 3)

Figure 3: CT scan neck with gastrographin swallow Sagittal cut. Showing loss of cervical lordosis denoting neck muscles spasm, widening of the prevertebral space due to edema and surgical emphysema. Ba leak into the retropharyngeal space (arrow) is noted at the level of upper border of C4. were done. They were transferred to the operating theater; external neck examination was done to locate the missals’ inlets and exits.Direct laryngeal examination was done under general anesthesia (GA) followed by tracheostomy and neck exploration through a wide U-shaped neck incision. Strap muscles were cut exposing the larynx and pharynx that were skeletonized and separated from the carotid sheath on both sides. Vascular injuries were managed when present by vascular surgeons. During neck exploration the assistant harvested the AFLG as follows; the thigh is flexed to a level that allows knee flexion of 90° while being supported from below with packed drapes. The leg is fixed to the table at 150° adduction of the hip joint. An “S”-shaped incision line is marked 6 cm proximal to the lateral femoral condyle. This incision enables the harvest of a 10 X 20 cm fascial sheath. A transverse incision is made through the fascia distally while two-tissue forceps are used to hold and fasten the fascia. The fascial sheath is cut longitudinally with slightly opened tips of scissors. Skin is closed in layers using subcutaneous interrupted 4/0 Vicryl sutures and skin staples. The Free non-vascularized AFLG is fashioned and tightly sutured using 3/0 vicryl suture to the posterior pharyngeal wall covering the whole pharyngeal tear and in mid line to avoid collection beneath the graft (Figure 4).

Figure 4: Free non-vascularized fascia lata flap sutured to the posterior pharyngeal wall covering the whole pharyngeal tear Pedicled sternomastoid flap was sutured to the posterior pharyngeal wall near the border of the fascia lata graft for better blood supply (Figure 5).

Figure 5: Superiorly pedicled vascularized sternomastoid muscle (SCM) flap(arrow) prepared to be sutured near the fascia lata graft
Strap muscles were approximated using 3/0 vicryl sutures, suction drain was applied and neck incision was closed in two layers. The patients were admitted to the ICU for 24 hours on NGT feeding that lasted for 10 days. Broad spectrum parenteral antibiotics together with Atropine Sulphate 0.6mg with 5 mg Pheneramine maleate incorporated in 500ml normal saline as intravenous drip (every 6 hours to decrease salivary secretions) were given for one week postoperatively. Fibro optic laryngeal examination was done seven days postoperatively to assess patency of the airway to begin tracheostomy weaning. Ten days postoperatively gastrographin swallow was done before discharge followed by CT scan of the neck one month later. Six months follow up visits showed neither symptoms nor signs of complications. The fourth case was a 4 years old child with history of metallic foreign body ingestion followed by rupture pharynx during extraction ending in a retropharyngeal abscess that was drained. He was also subjected to the same procedure as the previously mentioned cases except for a different dose of Atropine Sulphate and Pheneramine maleate(0.03mg/Kg every 6 hours and 1.5mg/Kg daily intramuscular injection respectively).
RESULTS
This study included four patients presented with different types of neck injuries and pharyngeal tears causing salivary leak. The cause of neck injury in three patients was gunshot injury while the fourth was due to metallic foreign body extraction. The diameter of the pharyngeal tears ranged between 23-10mm at its greatest dimension. The first case showed a 6 mm rounded darkly stained inlet of the missal at the right side of the neck at the level of the anterior border of sternomastoid muscle and a 9mm irregular rounded darkly stained exit behind the left shoulder just above the level of the clavicle pointing to injury from a near distance. Direct laryngeal examination under GA of this patient showed marked edema of the laryngeal inlet with blackish discoloration of the laryngeal and Hypopharyngeal mucosa. Neck exploration of this patient revealed a big right sided hematoma overlying injured right internal jugular vein. The hematoma was cleared and the internal jugular vein was trimmed with resection anastomosis using 6/0 prolene suture. This patient also had fractured transverse process of sixth cervical spine with no neurological deficits that required no surgical intervention. Marked edema, charring and tissue necrosis were seen in this patient in the space between the pharynx and the prevertebral muscles and fascia. No actual tear was scored in the pharyngeal wall but a ruptured posterior pharyngeal wall at multiple levels (dissection) was seen the level of the middle constrictor muscle in the mid line.
Second patient had an 18 mm pharyngeal tear, injured right internal jugular vein with small hematoma that required linear repair using 6/0 prolene suture. He also had fractured right ala of thyroid cartilage that was sutured using 3/0 prolene suture table 1.
Table 1: Patients’ age, clinical, surgical and radiological findings.
| No | Age in years | Cause of injury | Air way injury | Pharyngeal tear | Vascular injury | Bony injury | |||
| 1 | 36 | Gun shot | -ve | 23 mm | Right IJV | left TP of C6 | -ve | -ve | -ve |
| 2 | 26 | Gun shot | Thyroid cartilage injury | 18 mm | Right IJV | -ve | -ve | -ve | -ve |
| 3 | 19 | Gun shot | -ve | 20 mm | -ve | -ve | Left RLN | left VFP | -ve |
| 4 | 4 | Foreign body extraction | -ve | 10 mm | -ve | -ve | -ve | -ve | -ve |
Abbreviations: IJV: Internal Jugular Vein; RLN: Recurrent Laryngeal Nerve; VFP: Vocal Fold Paralysis
Our third case showed a 5 mm inlet at the anterior border of the left sternomastoid muscle and an irregular 7 mm rounded exit anterior to the border of the right trapezius muscle. Pharyngeal tear was 20 mm with neither vascular nor bony injuries but ended with left vocal fold paralysis due to recurrent laryngeal nerve injury that lasted for more than six months postoperatively. AFLG harvesting produced no functional deficits, and complications at the donor site were insignificant. All patients showed good response with no evidence of pharyngeal stenosis and complete closure of the pharyngeal tears that were proved clinically and radiologically.
DISCUSSION
The fascia lata is the deep fascia of the thigh – a veritable stocking forming an ectoskeleton for its muscles. It is a trilaminar fibrous tissue sheath that envelops the muscle groups-of the thigh. The attraction of using the fascia as an autograft stems from the sparsity of its cell populations and thus its low nutritional requirements [8].The commonest cause of pharyngeal perforation is iatrogenic (i.e., occurring during instrumentation) [9-11]. It has a more favorable prognosis than perforation caused by blunt trauma to the neck, in which the tear is usually larger or extends to the intrathoracic esophagus. Knowledge of the size and location are critical to the management of this injury. Most authorities believe that primary closure should be performed [11]. Pharyngo-esophageal injuries are a rare complication of anterior cervical spine surgery, these injuries occur intraoperatively from sharp instrumentation or retraction and are repaired acutely at the time of injury, and typically heal reliably without subsequent clinical sequelae [12]. Occult Pharyngo-esophageal perforations after cervical spine injury, penetrating or blunt trauma may lead to severe mediastinitis, sepsis, and death. Most of the Pharyngo-esophageal perforations can be repaired by double layer imbricating sutures that may be followed by strictures in up to 54% of cases [13]. A high incidence of fistula formation requiring tube feeding for several weeks to months has been reported following nonsurgical treatment of a pharyngo-esophageal leakage [14]. For few cases the use of local muscle flaps such as the sternocleidomastoid flap has been reported [15]. We were confronted with many cases with gun shots’ injuries in the head and neck, some of these injuries were lethal; others were successfully treated with neither morbidity nor mortality. Direct laryngeal examination of the first three cases under GA revealed severe edema of the laryngeal inlet that hindered proper assessment of vocal folds’ status. We managed three cases with gunshot injuries in the neck, all showed wide pharyngeal tears with irregular borders and dissection at multiple levels that can’t be repaired by primary sutures. Thus we didn’t prefer to use SCM flap alone, hence arose the idea of using free non-vascularized AFLG. The tough nature of the AFLG rendered it more tolerant and resistant to infection hence successfully used in the child with history of foreign body extraction and drained retropharyngeal abscess. Harvesting a wide AFLG covering the whole tear together with tight interrupted sutures ensures proper sealing and good healing of the tear. Owing to the sparsity of the cell populations and thus the low nutritional requirements of AFLG we used SCM flap as second layer to increase vascularity for proper healing. Although fibroptic laryngeal examination was nearly impossible in a stridulous, agitated patient with edematous and emphysematous neck, yet this can still be a pitfall in our study. This was clear in the third patient who developed left vocal fold paralysis of uncertain etiology. This raised the concept that this is a demanding technique with possible after effects that should be studied thoroughly in further studies. Early postoperative follow up was done on clinico-radiological basis that showed complete sealing of the tear with no evidence of stenosis or spill over. Long term follow up plan stipulated subjecting the patients to radiological evaluation only in the case of the emergence of complications namely; dysphagia, aspiration, regurgitation and/or fever. We think that inducing xerostomia using Atropine sulphate/Pheneramine maleate combination has given a great opportunity for good healing and graft take.
CONCLUSION
The use of non-vascularized AFLG is beneficial and gives good results in the repair of wide primary irreparable pharyngeal tears aided by pedicled SCM flap. Thus using the non-vascularized AFLG in primary repair of the neo-pharynx in larygectomized patients with irradiated neck is now under trial in the same center.








































































































































