Paravertebral Hydatid Cyst: A Case Report
- 1. Department of Pneumology, Hospital 20 Août 1953, Morocco
Abstract
Hydatidosis is an anthropozoonosis caused by the development of cysts corresponding to the larval form of a taenia called Ecchinococcus granulosis. Bone hydatidosis is rare, accounting for only 0.9% to 2.5% of all cases. We report the case of a 41-year-old woman who was admitted to the Pneumology Department on hospital 20 Aout at Casablanca, Moroocco with symptoms consisting mainly of hemoptysis and hydatid vomiting. Lesion assessment revealed three left pulmonary cysts associated with a cystic formation in the left paravertebral gutters. Treatment was medico-surgical.
Keywords
Hydatid cysts, Parasitic disease, Paravertebral localisation, IRM
Citation
Arfaoui H, Zadi M, Msika S, Jabri H, El Khattabi W, et al. (2023) Paravertebral Hydatid Cyst: A Case Report. Clin Res Pulmonol 9(2): 1060.
INTRODUCTION
Hydatid cysts are a fairly common parasitic disease in endemic countries. It frequently occurs in the liver and lungs. Paravertebral hydatidosis is a rare localization of bone echinococcosis [1,2]. The cyst can cause spinal cord compression, in general the clinical examination is poor. On the paraclinical level, CT and MRI have an essential role We report the observation of a patient presenting with a paravertebral cyst with pulmonary cysts.
PATIENT AND OBSERVATION
The patient was 41 years old, married, mother of two children, housewife, living in a rural area of Benimellal in Morocco, having contact with dogs, treated for pulmonary tuberculosis in 2002. She consulted the pneumology department for a symptomatology consisting of three episodes of hemoptysis of low abundance and one episode of hydatid vomiting, associated with dyspnea stage II mMRc without chest pain or neurological signs, in a context of febrile sensations, night sweats and general decline in condition. Clinical examination revealed diminished vesicular murmurs in the left basithoracic region with systolic murmur at the mitral focus and dorsal scoliosis. Chest X-ray showed a left supra- and subclavicular opacity dotted with clearness, with blunting of the left pouch over a retracted left hemithorax.
Thoracic CT revealed three left lung cysts associated with cystic formation in the left paravertebral gutters at the level of vertebrae D10-D12, eroding the cortex of the vertebral bodies, the corresponding transverse apophyses and ribs, extended intra-canal with lysis of the posterior arch of D10 and a calcified cyst of the hepatic dome. Flexible bronchoscopy showed complete obstruction of the left lower lobar by whitish membranes that were difficult to remove, with no other visible abnormalities. The bronchial aspiration fluid was tested positive for scolex, as was hydatid serology. Cerebral CT, abdominal ultrasound and cardiac ultrasound revealed no cystic images. The diagnosis was multiple pulmonary hydatidosis, including one paravertebral and one calcified hepatic hydatid cyst. Treatment consisted of concomitant resection of the pulmonary hydatid cysts and the paravertebral hydatid cyst [Figure 4],
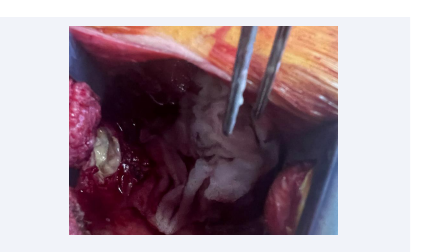
Figure 4: Opening of the internal capsule of multiple cysts and vesicles, and evacuation of the contents.
with firstly a left lobectomy under right posterolateral thoracotomy and secondly an anterior approach to the left paravertebral mass at D10-D11. The procedure consisted in opening the capsule of multiple cysts and evacuating the collection, as well as extracting multiple vesicles and KH and washing abundantly with hypertonic serum. Albendazol-based medical treatment was administered pre- and postoperatively. The patient remained in intensive care for 07 days, then was transferred to the thoracic surgery department with a simple postoperative course. The patient progressed well, with resolution of haemoptysis and dyspnoea. The particularity of our observation is the paraspinal localization of the hydatid cyst, with good evolution under medical-surgical treatment.
DISCUSSION
Hydatid disease is a public health problem in endemic countries, including Morocco. Hepatic and pulmonary localizations are the most frequent. Bone hydatidosis accounts for 2% of all cases of hydatid disease [3]. Paravertebral localization remains very rare, accounting for around 2.2% of all bone hydatid cysts. The thoracic spine was most frequently affected, followed by the lumbar region, and exceptionally the cervical region [3,4]. Thoracic vertebral involvement is more frequent in men than in women, with an average age of 33.5 years [3]. The hexacanth embryo passes from the digestive tract into the portal system, successively passing through the hepatic and pulmonary filters before settling in the skeleton, resulting in primary bone echinococcosis. This explains the rarity of bone localizations compared with those of the liver and lungs [5]. Secondary bone invasion from primary soft tissue involvement is possible [5]. Paravertebral hydatid cysts shows no pathognomonic signs or symptoms other than those related to spinal cord compression, it may be the cause of spinal pain, muscle weakness, vertebral fractures or micturition disorders [7,8].
In our patient, the paravertebral hydatid cyst was asymptomatic, discovered on thoracic CT [Figure 1 and Figure 2].
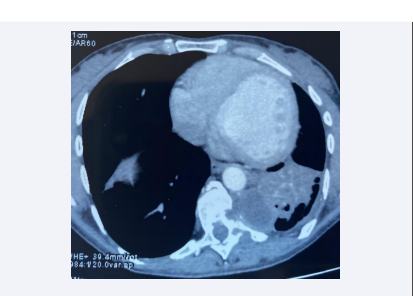
Figure 1: Frontal section of thoracic tdm showing left pulmonary hydatid cysts with a homolateral paravertebral hydatid cyst
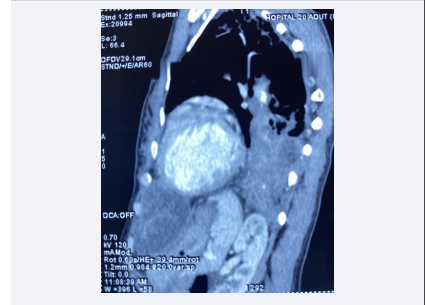
Figure 1: Sagittal section of thoracic tdm showing left pulmonary hydatid cysts with a homolateral paravertebral hydatid cyst.
Diagnosis of paravertebral hydatid cysts is generally based on medical imaging, mainly computed tomography (CT) or magnetic resonance imaging (MRI). The latter is the most effective examination for visualizing the cyst, determining its size and exact topography, and studying lesion relationships with nerve structures and the meninges [6]. Certain MRI signs are pathognomonic of echinococcosis, such as the hypointense nature of the cystic wall on T1- and T2-weighted sequences [9] (Figure 3).
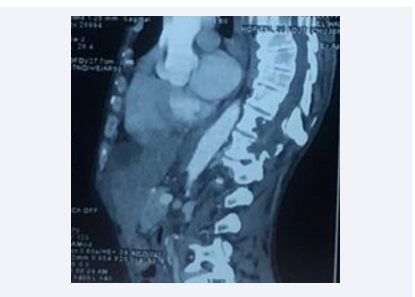
Figure 3: Sagittal section of spinal cord MRI showing multiple vertebral and paravertebral cystic formations at D9, D10 and D11 with endocanal extension.
Paravertebral hydatid cysts are treated medico-surgically. The aim of medical treatment is to reduce the size of the cysts, sterilize their contents preoperatively and postoperatively to treat small cysts that have passed into view [6,10]. Surgical treatment consists of “carcinological” excision of the lesions, which are likened to a true malignant tumour, with complete removal of the hydatid lesions, but despite the various therapeutic methods, relapse rates after partial excision are very high [11,12]. This procedure can be difficult because of close anatomical connections [11,12]. Prognosis is dominated by endocanal involvement, and depends on early diagnosis and surgical intervention [11]. Prevention of paravertebral hydatid cysts involves individual and collective preventive measures.
CONCLUSION
Paravertebral hydatidosis is a rare localization, even in endemic areas. It is difficult to diagnose because of its insidious course. The prognosis can be critical, hence the importance of individual and collective prevention.
Contributions of the Authors
Hajar Arfaoui: Responsible professor and 1st author; Meryem Zadi: Attending doctor and 2nd author; Salma Msika: Resident doctor; Hasna Jabri: Responsible professor; Wiam Elkhattabi: Responsible professor; Hicham Afif: Head professor. All authors contributed to this work. They have read and approved the final version of the manuscript.
RÉFÉRENCES
2. Kystes hydatiques compliqués du poumon Rév Mal Respir (2009).
4. Argenson C, Riffet J, Lacour C. Hydatidose vertébrale à propos de 2 cas. Rev chir Orth. 1989; 75: 267–270.
9. Bondiau PY, Peyrade F, Birswitle I, Thyss A, Bruneton JN. Hydatidose osseuse : aspect pseudo-sarcomateux. Presse Med. 1993; 22: 367.
11. Louis R., Casanova J., Baffert M. Techniques chirurgicales des tumeurs du rachis. Rev. Chir. Orthop. 1976; 62: 57.







































































































































{kind=link}