Pulmonary Process Revealing a Follicular Thyroid Tumor- A Case Report
- 1. Department of Pneumology Department, Hospital 20 Août 1953, CHU Ibn Rochd, Casablanca, Morocco
Abstract
Metastases from follicular thyroid carcinomas are rare. Thoracic metastases mainly involve the lungs, mediastinal lymph nodes and pleura. We report a case showing the natural course of follicular thyroid cancer in a female patient aged 66, exposed to passive smoking, known hypertensive and type 2 diabetic, with a 46-year-old goiter refusing all management, who reported a right interscapulo-vertebral burning pain associated with mucous bronchial syndrome and stage II mMRC dyspnoea. Clinical examination revealed laryngeal stridor associated with the presence of 3 cervical masses. The chest X-ray showed a right laterotracheal opacity associated with a cannon ball appearance and bone lysis opposite the 3rd, 4th and 5th ribs. Cervico-thoracic CT scan showed 2 plunging right and left thyroid masses associated with bilateral laterocervical adenopathies and a right apico-dorsal tissue process with costal lysis, parietal and vertebral invasion associated with a cannon ball appearance and mediastinal adenopathies. Histological study revealed a secondary localization of a follicular thyroid tumor. Only decompressive radiotherapy was indicated, with surgical and iratherapy abstention in view of the patient’s advanced stage.
Keywords
• Pulmonary Process ; Thoracic Metastases ; Follicular Thyroid Tumo ; Metastatic Cannon Ball
CITATION
Hallouli S, El Khattabi W, Bamha H, Bougteb N, Arfaoui H, et al. (2024) Pulmonary Process Revealing a Follicular Thyroid Tumor- A Case Report. Clin Res Pulmonol 10(1): 1067.
INTRODUCTION
Metastases from follicular thyroid carcinomas are rare. Thoracic metastases mainly involve the lungs, mediastinal lymph nodes and pleura. We report a case showing the natural course of follicular thyroid cancer in a patient with a 46-year-old goiter refusing all management, who presented with a right lung mass and a metastatic cannon ball appearance.
Patient and Observation
Mrs E.R aged 66, exposed to passive smoking for 39 years, known hypertensive and type 2 diabetic for 4 years on treatment, poorly followed for a goiter for 46 years (surgery indicated but refused by the patient). She reported the progressive onset of right interscapulo-vertebral burning pain associated with mucous bronchial syndrome and stage II mMRC dyspnoea for 4 months, evolving in a context of apyrexia and preservation of general condition. Clinical examination revealed laryngeal stridor associated with the presence of 3 cervical masses (Figure 1) measuring 13 cm, 5 cm and 3 cm in diameter respectively, fixed, painless and with no lower limit. Pleuropulmonary examination was essentially normal.
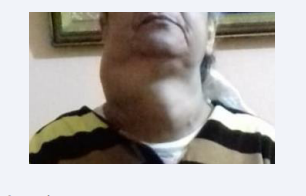
Figure 1: Clinical examination showing 3 cervical masses.
The chest X-ray (Figure 2) showed a dense, inhomogeneous right laterotracheal opacity with sharp contours, gently sloping into the mediastinum, with decreased transparency of the upper third of the right hemithorax, bone lysis adjacent to the 3rd, 4th and 5th ribs and multiple diffuse nodular opacities in both lung parenchyma, creating a cannon ball appearance.
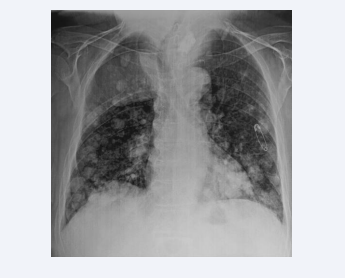
Figure 2: Front thoracic X-ray showing a right laterotracheal opacity associated with a cannon ball appearance and bone lysis opposite the 3rd, 4th and 5th ribs.
A cervicothoracic CT scan (Figure 3) showed a plunging right thyroid mass of tumoral appearance, very heterodense with several areas of necrosis, compressive and pushing the larynx and trachea to the left; another plunging left thyroid mass with micro and macro calcifications, pushing the trachea to the right; and multiple bilateral laterocervical enlarged lymph nodes of metastatic appearance.
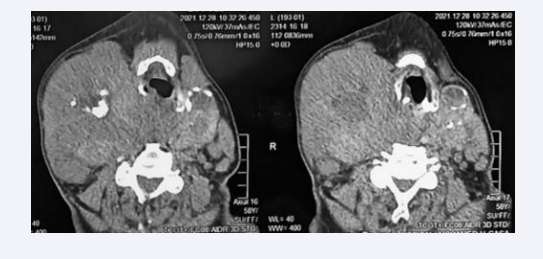
Figure 3: Cervical level of cervicothoracic CT scan showing 2 plunging right and left thyroid masses associated with bilateral laterocervical adenopathies.
On the thoracic level (Figure 4), there was a right apico-dorsal tissue process with costal lysis opposite, parietal and vertebral invasion associated with multiple nodules scattered over both lung fields, giving a cannon ball appearance, and pre vascular mediastinal, Barety’s lodge, aorto-pulmonary window and left hilar enlarged lymph nodes.
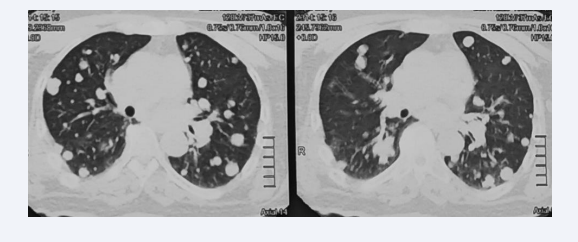
Figure 4: Thoracic level of cervicothoracic CT scan showing a right apico-dorsal tissue process with costal lysis, parietal and vertebral invasion associated with a cannon ball appearance and mediastinal adenopathies
The patient’s thyroid workup was normal, with TSH at 2.1 mIU, T3L at 2.1 umol/L, T4L at 14 pmol/L. In the absence of flexible bronchoscopy, which was difficult to perform because of the cervical masses and refused by the patient, a transparietal biopsy of the right apico-dorsal process revealed on histological study a secondary localization of a follicular thyroid tumor (Figure 5).
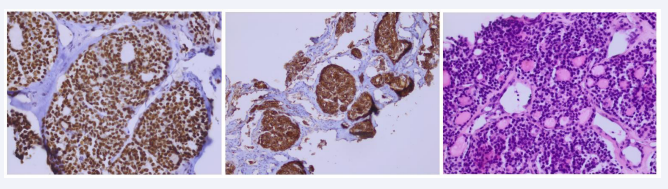
Figure 5: Histological study of transparietal biopsy, showing fibrous tissue infiltrated by an endocrine tumor proliferation, partially follicular.
The patient refused to undergo thyroid biopsy, and cytopuncture revealed a follicular thyroid tumour (Bethesda category IV). After multidisciplinary consultation meetings, only decompressive radiotherapy was indicated, with surgical and iratherapy abstention in view of the patient’s advanced stage. The patient refused all organic or psychological treatment and was lost to follow-up.
DISCUSSION
Thyroid cancer is a relatively rare disease with a good prognosis, representing 1% of all cancers, and is predominantly female (76% of cases). Micro- or macronodular pulmonary metastases occur in 10-15% of cases, including papillary carcinoma in 70%, follicular carcinoma in 15%, and medullary and anaplastic carcinomas, which are rare [1].
Thyroid cancer metastases to the thorax via 2 main routes: the lymphatic route via the intrapulmonary and pleural lymphatics, and the hematogenous route via the pulmonary arteries (most frequent) and bronchial arteries (rarer) [2].
Clinical presentation is non-specific, and may include dry cough, bronchial syndrome, hemoptysis, chest pain, respiratory distress, stridor or dysphonia [3].
Thoracic metastases may be pulmonary, mediastinal lymph node or pleural. Pulmonary metastases are the most common form of thyroid cancer, particularly in differentiated cancers. They take the form of pulmonary nodules and micronodules, giving a cannon ball or miliary appearance, or calcifications. They are sometimes only visible on iodine-131 scintigraphy.
Positive diagnosis is mainly based on histology, using bronchial or transbronchial biopsies taken during flexible bronchoscopy, transparietal biopsy, pleural biopsy or surgery (mediastinoscopy or thoracoscopy) [4].
Lymph node metastases are mainly seen in papillary cancers. They have little or no sensitivity to radioactive iodine. Lymph node dissection is the standard treatment. Picking, or simple removal of one or more lymph node metastases, is not recommended. Metastases may be synchronous, contemporaneous with the thyroid tumour, or metachronous, appearing at a distance from the treatment of the thyroid tumour [5].
Pleural metastases are rare, presenting as recurrent pleurisy, nodules and pleural masses. They are confirmed histologically by pleural biopsy, transparietal biopsy or thoracoscopy. Their prognosis is poor. Iratherapy is ineffective, and treatment is palliative with chemotherapy and pleurodesis, which is indicated for recurrent pleural effusions [5].
Progression is variable, ranging from complete remission to rapid progression and death [3].
Minimally invasive follicular carcinoma has a good prognosis, with a risk of long-term death in 3 to 5% of cases, whereas widely invasive follicular carcinoma has a much more guarded prognosis, with a risk of long-term death of around 50, and a much greater risk of distant metastases.
Prognostic factors include age at diagnosis, tumor histology, site of metastasis and avidity of iodine-131. The 10-year survival rate is 25-70% [3].
CONCLUSION
This study highlights the importance of screening for thyroid tumour pathology at an early stage, in order to reduce the risk of metastatic disease, particularly in the thoracic region, which is particularly detrimental. It also underlines the importance of psychological management of patients suffering from the disease, since the organic and psychological aspects must be appreciated, differentiated and treated with the same rigour.
Contributions of the Authors
Soukaina Hallouli: Attending doctor and first author ; Wiam Elkhattabi: Responsible professor and second author;; Hajar Bamha: Attending doctor and third author ; Nabil Bougteb: Responsible professor; Hajar Arfaoui: Responsible professor; Hasna Jabri: Responsible professor; Moulay Hicham Afif: Head professor.
All authors contributed to this work. They have read and approved the final version of the manuscript.
REFERENCES
5. Référentiels OncoCentre - Cancers de la thyroïde. 2015.









































































































































{kind=link}