Neuronal Cells Damage and Stroke in a Female Following Snake Bite
- 1. Department of Medicine, Maharani Lakshmi Bai Medical College, India
Abstract
Ischemic stroke following snake bite is rare. We report a case of a 45 years old female developing hemorrhagic manifestations and left sided hemi paresis following a snake bite (unknown species). MRI brain shows multiple acute brain infarct/ toxic leukoencephalopathy in infratentorium and suoratentorium with surrounding mass effect and possible neuronal cells death. Most common and serious central nervous system complication following snake bite is intracranial hemorrhage. Ischemic stroke commonly involves anterior circulation. Bilateral cerebellar and occipital infraction is not yet reported in literature. Exact cause for the development of infarction is not clear. The possible mechanisms of infarction in this scenario are discussed.
Citation
Singh RB, Kumar A (2014) Neuronal Cells Damage and Stroke in a Female Following Snake Bite. JSM Cell 2(1): 1009.
Keywords
Stroke; Snake bite; Neuronal damage; MRI study.
ABBREVIATIONS
MRI: Magnetic Resonance Imaging; ASV: Anti Snake Venom
INTRODUCTION
Snake bites are common cause of morbidity and mortality in India. On an average, 200 000 fall prey to snake bite per year in India, and an estimated mortality may range from 20 000 to 50 000 cases. Viperidae species consisting of Russell’s viper (Daboia russelli) and saw scaled viper (Echis carinatus) are the leading cause of fatal snake bite in India. The common clinical characteristics of viper bite include local cellulites, renal failure, and systemic hemorrhagic manifestation. Neurological deficit following viper bite is not uncommon and is usually due to intracerebral or subarachnoid bleed. Ischemic infarction following viper envenomation has been described by only few authors. In majority of the cases reported, ischemic infarction involved the anterior circulation. Korean viper bite resulting in brain stem infarction has also been reported.
CASE REPORT
45 years old patient, Kala Yadav, had a snake bite on her left leg on 16th oct, 2013 at around 3 pm. Followed by which she developed severe pain, local swelling, and mild ptosis. She was brought to our hospital around 6.30 pm on the same day with her blood pressure of 116/70 mmHg, pulse rate of 20/min, mild ptosis, single breath count was 17 , respiratory efforts were good and 20 mins whole blood clotting test was positive [1-10].
She was given primary management accordingly and was given 10 vials of polyvalent Anti Snake Venom (ASV). At this time there was no apparent hemorrhagic manifestation. On investigations Hb 14.4, Hct 43.1, Platelet count was normal, CT, BT, PT/INR, APTT, ABG, electrolytes are within normal limits. Urine shows hematuria and pus cells. MRI BRAIN shows Multifocal acute brain infarct/ toxic leukoencephalopathymin infratentorium and supratentorium with surrounding mass effects (Figure 1).
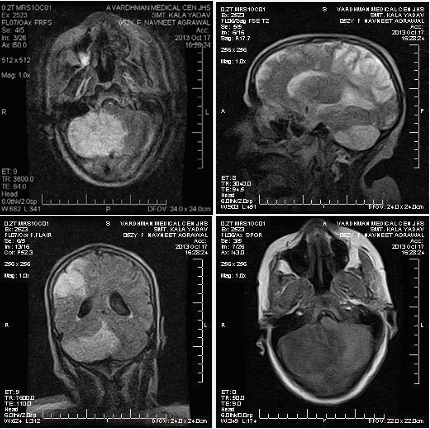
Figure 1: MRI of the brain showing different regions showing encephalopathy.
Large right cerebellar hemispheric infarct with mass effect and compression of 4th ventricle upstream, mild hydrocephalus with dilation of lateral and 3rd ventricle and mild tonsillar herniation
A patient was managed with ASV, blood transfusions, broad spectrum antibiotics, mannitol. The patient finally died next day.
DISCUSSION
Viper snake venom is a complex toxin with rich components affecting hemostatic mechanisms. Most of the viper venom exhibit both anticoagulant and coagulant effects. In large doses, venom can cause massive intravascular coagulation, leading to occlusion of small and even large vessels resulting in cerebral infarction. Toxic vasculitis caused by certain viper species may result in thrombosis.
Possible mechanism may be:
- Hypercoagulation due to procoagulants in venom, such as arginine, esterase, and hydrolase.
- hyperviscosity caused by hypovolemia and hypoperfusion secondary to hypotension.
- Endothelial injury due to toxic vasculitis by the components of venom can lead to thrombosis.
- Neuronal cell death because of ischemia and lack of oxygen and other nutrients supply to the neurons.
The infarcts in our patient are not in a classical watershed territory and therefore do not suggest hypotension as a cause. Clotting time was normal and ruled out coagulapathy as a cause. The possible cause of infarct in the posterior circulation is due to toxic vasculitis caused by injury to the endothelium by snake venom toxin.









































































































































{kind=link}