Causes of Maternal Mortality in Delta State University Teaching Hospital, Nigeria: A Retrospective Study
- 1. Department of Family Medicine, Delta State University, Abraka, Delta State, Nigeria.
- 2. Department of Statistica Sciences, Sefako Makgatho Health Sciences University, Pretoria, South Africa
Abstract
Background: Maternal deaths remain excessively high in developing countries, particularly in sub-Saharan Africa. In Nigeria, the Maternal Mortality Rate (MMR) ranged from 448 to 4210 per 100,000 live births with hypertensive disorders and haemorrhage as common causes. The aim of this study was to determine MMR and causes of maternal death in the Delta State University Teaching Hospital.
Methods: A retrospective descriptive study was conducted at Delta State University Teaching Hospital, Nigeria (January 1, 2014 to December 31, 2018). The hospital deaths register was used as the starting point in the collation of a list of all maternal deaths and relevant maternal death medical records were retrieved and reviewed. The following information was extracted: date of death, age, ethnicity, referring facility, place of death and cause of death. The STATA® 16.1 (StataCorp; College Station, USA) was used for statistical analysis.
Results: There were 788 live births with a total of 57 maternal deaths resulting in MMR of 7,234 per 100,000 live births during the study period. The mean age of the women was 30.4 ± 7.3 years ranging from 15 to 46 years, with majority of women (53%) aged ≥ 30 years, 96% being referred and 18% delivered by caesarean sections. Overall, direct causes were responsible for 80% (n = 44) of all deaths, with hypertensive disorders in pregnancy 45% (25/55), medical/surgical conditions 15% (8/55) and obstetric haemorrhage 13% (7/55) being the most prevalent maternal cause of deaths.
Conclusion: Maternal deaths are unacceptably high in this hospital, and associated with direct obstetric causes which include hypertensive disorders in pregnancy and haemorrhage. Improvement in quality antenatal care, timely identification of the cause of obstetric haemorrhage and access to blood products are an important intervention in the reduction of maternal deaths in this tertiary hospital.
Keywords
Maternal mortality, Pregnancy, Delta state, Nigeria
Citation
Clark C, Ntuli ST (2023) Causes of Maternal Mortality in Delta State University Teaching Hospital, Nigeria: A Retrospective Study. J Family Med Community Health 10(1): 1190.
INTRODUCTION
Deaths related to pregnancy and childbirth remain a major public health challenge worldwide particularly in low and middle income countries. In 2015, there were 303,000 maternal deaths worldwide, of which the greatest number occurred in sub-Saharan Africa and South Asia.1 Even though there was a 44% reduction in MMR between 1990 and 2015 worldwide. The decline did not reach the United Nation Member States target of 75% by the end of 2015 [1]. The aim, therefore, is to reduce the global MMR to less than 70 deaths per 100,000 live births by 2030 as part of the Sustainable Development Goal (SDG) [2]. Several community and hospital based-studies in sub-Saharan Africa reported relatively high MMR ranging from 448 to 4,210/100,000 live births in Nigeria [3-7], 128 to 357/100,000 live births in Ghana [8], 650 to 1,579/100,000 live births in South Africa [9,10], and 1,541/100,000 live births in Tanzania [11], whereas in India, the ratio was 410/100,000 live births [12].
The main causes of maternal deaths in developing countries were direct causes, mainly hypertensive disorders in pregnancy and obstetric haemorrhage [4,5,12-16], while in developed countries, infection followed by hemorrhage and hypertensive pregnancy disorders accounted for the majority of maternal deaths [16]. In contrast, in rural South Africa, studies found indirect causes mainly HIV/AIDS infections the leading causes of maternal deaths [9,10]. Other risk factors linked with maternal death in developing countries include advanced maternal age, poverty, low levels of education, lack of antenatal care and multiparity [3,5,7,9,14,16,18]. There is little or no information on the MMR from Delta State University Teaching Hospital (DELSUTH) in Nigeria. Therefore, this study was undertaken to determine the magnitude of MMR and identify the underlying causes of maternal mortality in this referral tertiary hospital from January 1, 2014 to December 31, 2018.
METHODOLOGY
This was a retrospective descriptive study based on the review of maternal records at DELSUTH located in Oghara, Nigeria. The hospital has a maximum of 180 beds with 11 beds in Labour Ward and 2 in High Dependency Unit (equivalent to intensive care). Data for this study was collected over a five-year period, from January 1, 2014 to December 31, 2018. A data collection tool designed for the study was used to collect the data. The registry of hospital deaths and maternity register were used as the starting point for collecting the data of all maternal deaths that occurred during the period of the study. Appropriate maternal case notes for all pregnant women who died in the maternity ward and High Dependency Unit (equivalent to intensive care) were retrieved and checked and the following information was gathered: date of death, age, ethnicity, referral facility, method of delivery, place of death and probable cause of death. The STATA® version 16.1 for Windows (StataCorp; College Station, USA) was used for statistical analysis. Descriptive statistics such frequencies and mean ± Standard Deviation (SD) were used to interpret categorical and continuous variables, respectively. Ethical clearance was granted by DELSUTH’s Health Research Ethics Committee (HREC) (Ref: HREC/2018/057/0354) and DELSUTH Management granted permission to access hospital registers.
RESULTS
During the study period, a total of 57 maternal deaths were reported, giving an MMR of 7,234 per 100,000 live births. Annual MMRs with the worst ratio observed in 2015 and 2018 are shown in (Table 1).
Table 1: Maternal Mortality Ratio in DELSUTH (2014-2018).
| Year | Number of live birth | Number of Maternal deaths | MMR/100,000 |
| 2014 | 268 | 9 | 3,358 |
| 2015 | 137 | 18 | 13,139 |
| 2016 | 120 | 5 | 4,167 |
| 2017 | 155 | 8 | 5,161 |
| 2018 | 108 | 17 | 15,741 |
| 2014-2018 | 788 | 57 | 7,234 |
The mean age of the women varied between 15 and 46 years and was 30.4 ± 7.3 years. Just over half (53 percent) were 30 years of age and older. The age distribution of women who died during the study period is shown in (Figure 1).
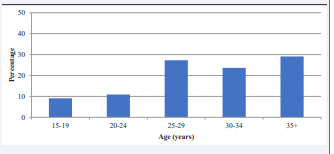
Figure 1: Age distribution of maternal deaths.
The rate of caesarean section was 18%, with most of the women 96% (n = 53) being referred [regional (n = 10) and district (n =43) hospitals]. Eighty-four per cent of maternal deaths occurred in the High Dependency Unit.
The major causes of maternal mortality were direct causes accounting for 71% (n = 44) of all deaths, whereas indirect causes accounted for 21% (n = 12). The cause of death for one woman was unknown. The most prevalent maternal cause of death was hypertensive disorders in pregnancy, accounting for almost half 44% (25/55) of all maternal deaths, followed by medical/surgical conditions and obstetric haemorrhage, resulting in 18% (10/55) and 12% (7/55) of all deaths, respectively. (Table 2)
Table 2: Causes of maternal deaths in DELSUTH (2014-2018).
| No | % | |
| Direct Causes | 44 | 71 |
| Hypertensive disorders in pregnancy | 25 | 57 |
| Obstetric Haemorrhage | 7 | 16 |
| Puerperal Sepsis | 6 | 14 |
| pulmonary oedema | 3 | 7 |
| Other | 3 | 7 |
| Indirect Causes | 12 | 21 |
| Medical/Surgical conditions | 10 | 83 |
| Non-pregnancy related infection | 2 | 17 |
| Unknown | 1 | 2 |
presents the underlying maternal causes of death during the period of study.
DISCUSSION
The maternal mortality ratio from this study was 7,234 per 100,000 live births which is higher than the ratio recorded in some tertiary health facilities in Nigeria (448 to 4210 per 100,000 live births) [3-7], and 128 to 357 per 100,000 live births in hospital and community-based studies in Ghana.8 The ratio is also higher than 650 to 1,579 per 100,000 live births reported in South Africa [9,10], 1,541 per 100,000 live births in Tanzania [11] and 410 per 100,000 live births in India [12]. In this analysis, the explanation for high MMR is not clear, but the drastic increase observed in 2015 and 2018 is multifactorial [14]. This could have been due to the industrial strikes by healthcare workers during that time [19,20].
In order to reduce maternal mortality in Nigeria particularly in this referral tertiary facility, it is important to identify the high risk groups for the development of intervention programs. Slightly more than half (53%) of maternal deaths in our study happened in women in the age group ≥ 30 years. Previous studies have reported similar results [9,16], but they vary from several studies that have found deaths in those below 30 years of age [5,13,15,21]. Poverty, low levels of education, lack of antenatal care and multiparity could have been the reasons for the higher number of maternal deaths in women aged 30 years or older in our research [3,5,7,9,14,16,18]. Not surprisingly, most (96%) maternal deaths occurred in women referred from regional and district hospitals in our research; and this is in line with a study conducted in South Africa [9]. While the time at which deaths occurred was not determined by our research, multiple studies performed in tertiary hospitals showed that the majority of maternal deaths occur within 24 hours of admission [6,9]. Late referrals and a shortage of sufficiently trained staff in peripheral hospitals may be the explanation for this.
Regarding the cause of deaths, the major causes of maternal deaths were direct causes in our study (80%), with the leading causes being hypertensive pregnancy disorders and obstetric haemorrhage. Puerperal sepsis and pulmonary oedema were other direct causes of maternal deaths. This result is consistent with other retrospective studies conducted in Nigeria [4, 5,13,14]; Tanzania [15]; Pakistan [16] and India [12] which also reported direct causes mainly eclampsia and obstetric haemorrhage. Infection, bleeding, and hypertensive pregnancy disorders accounted for 60-70% of maternal deaths in developed countries [17]. In their report, however, Ntuli et al highlighted and complemented the marked decrease (18%) in MMR as a result of improved Highly Active Antiretroviral Therapy (HAART) uptake in HIV/AIDS management and non-pregnancy-related infections in South Africa.
In some reports from Nigeria, malaria during pregnancy was an indirect cause of maternal death [5,6], although in our research, there were no malaria-related maternal deaths which could be attributed to preventive treatment among pregnant women visiting antenatal care clinics [22-24]. One of the most serious problems found in our research is bleeding during or after the caesarean section, as suggested by around 18% of women who died after undergoing the caesarean section. In Latin America, a systematic analysis indicated an increased risk of cesarean section maternal mortality relative to vaginal delivery. In South Africa, 17.9% of the 1,243 mothers who died during or after caesarean section died as a result of haemorrhage during and after the procedure [26]. Maternal deaths are multifactorial., but can be minimized by improving healthcare workers’ skills and knowledge and rapid effective response to obstetric emergencies [27].
STUDY LIMITATIONS
It may not be possible to generalize the results of this research as it was based on only one tertiary hospital operating as a referral centre for the entire state. Moreover, evidence on the causes of death was compiled retrospectively from labour ward, HDU databases and patient records which may be vulnerable to misreporting of demographics and cause of death [28].
CONCLUSION
The findings from this study revealed that maternal mortality is unacceptably high in this tertiary hospital, and is associated with direct obstetric causes which include hypertensive disorders in pregnancy and obstetric haemorrhage. Therefore, this study concluded that improvement in quality antenatal care, timely identification of the cause of obstetric emergencies are important factors in the reduction of maternal deaths in this tertiary hospital.
ACKNOWLEDGEMENTS
Thanks to DELSUTH’s Record Division and Maternity staff especially Sr Ukecha for their assistance during this research. We are grateful to those who have made helpful suggestions and recommendations.
REFERENCES
21. Sandhya Devi KVSM, Madhuri Ch, Sarada Bai K,Srividya D. Study of maternal mortality in a tertiary care hospital. J Evol Med Dent Sci. 2015; 4(38): 6624-66230. doi:10.14260/jemds/2015/959.








































































































































{kind=link}