Metastatic Malignant Melanoma of Unknown Primary Presenting in an Inguinal Lymph Node: A Case Report
- 1. Department of Family Medicine, St Joseph Mercy Oakland, United States
Abstract
Background: Metastatic malignant melanoma of unknown primary is a rare diagnosis defined as a metastatic melanoma discovered first in the lymph nodes, subcutaneous tissue, or viscera without a known identifiable primary site.
Case Presentation: A 43-year-old female with a significant past medical history of pre-malignant skin lesions initially presented to the family medicine practice complaining of a swollen, non-tender left inguinal lymph node that she noticed a month prior. History was negative for fever, weight loss, night sweats or loss of appetite. Ultrasound showed left inguinal lymphadenopathy and heterogeneity. CT imaging showed additional lymphadenopathy in the left external iliac chain and no retro-peritoneal adenopathy. She underwent surgical excision. Grossly appearing on resection as hyperpigmented. Pathology determined it as metastatic melanotic melanoma. Additional skin survey done by melanoma clinic did not show primary lesion which ultimately led to her diagnosis of melanoma of unknown primary.
Conclusion: This clinical case report highlights an unusual manifestation of melanoma. Presentation of this case is to facilitate in future diagnose. Due to its rarity, metastatic malignant melanoma of unknown primary is understudied with no clear etiology, prognosis, or well-understood treatment implications for these patients. Additional research is crucial to understanding this disease process in order to more effectively identify patients at risk and approach treatment options.
Keywords
- Dermatology
- Lymph node excision
- Malignant melanoma
- Melanoma
- Rare diseases
- Skin neoplasms
Citation
Bargoti-Gosey Y, Gosey D, Singh R, LaJoie J (2020) Metastatic Malignant Melanoma of Unknown Primary Presenting in an Inguinal Lymph Node: A Case Report. J Family Med Community Health 7(3): 1180.
ABBREVIATIONS
MUP: Melanoma of Unknown Primary
INTRODUCTION
Malignant melanoma is one of the only remaining cancerswith an increasing incidence rate. Melanoma is responsible for a 2% annual increase in mortality and morbidity [1] and accounts for 1-2% of cancer deaths worldwide [2]. For this reason, early detection and treatment are crucial to improving prognosis. However, melanoma with an unknown primary site may present a unique challenge for detecting melanoma early.
Melanoma of unknown primary (MUP) is defined as a metastatic melanoma discovered first in the lymph nodes, subcutaneous tissue, or viscera without a known primary site. Most often, MUP presents in the lymph nodes with up to 16.6% of patients with MUP in any location presenting with a palpable lymph node [3]. MUP only appears in 3.2% of patients diagnosed with melanoma [4]. Due to its rarity, it is understudied with no clear etiology, prognosis, or well-understood treatment implications for these patients.
CASE PRESENTATION
A 43-year-old female with a significant past medical history of pre-malignant skin lesions initially presented to the family medicine practice complaining of a swollen, non-tender inguinal lymph node that she noticed a month prior. History was negative for fever, weight loss, night sweats or loss of appetite. Vitals were stable on presentation. On physical exam a 2.5 cm left inguinal lymph node was palpated. At that time, CBC with differential, urinalysis, CMP, ANA with reflex, CRP, sedimentary rate and ultrasound of the groin were ordered. All test results were within normal limits, aside from WBC count which was low at 4.4. Ultrasound showed an enlarged, heterogenous left inguinal lymph node that was 2.8x1.7x2.8 cm (Figure 1).
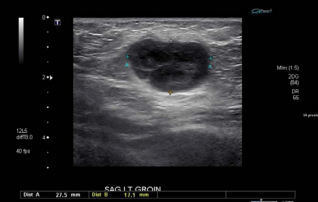
Figure 1 Ultrasound showing left inguinal lymph node measuring 2.8x1.7x2.8 cm (2019).
The patient consulted the family medicine physician several weeks later stating that the lymph node had not decreased in size and requested a CT scan. CT abdomen/pelvis showed a left inguinal lymph node measuring 2.5 x 2.8 cm that was morphologically abnormal (Figure 2).

Figure 2 PET CT showing inguinal lymph node of concern (2019).
The CT also noted a non-specific 0.9 cm lymph node along the left external iliac chain and no retro-peritoneal adenopathy (Figure 2). The patient was then referred to general surgery for further evaluation and excision was recommended.
Surgery reported that the lymph node was grossly pigmented and was sent to pathology which confirmed metastatic malignant melanoma. The patient presented 10 days post-operative complaining of fatigue, loss of appetite, and vomiting. At this time, full body PET scan and full body MRI was warranted to further understand the origin and etiology of the melanoma. The full body PET CT showed additional prominent lymph nodes and brain MRI was negative for metastasis. The patient was then referred to University of Michigan Multidisciplinary Melanoma Clinic. It was recommended that the patient undergo dissection of the left inguinal lymph nodes at that time.
After thorough inspection, no primary lesion was identified. On no occasion was the patient found to have a primary lesion. In the past, the patient had annual dermatology surveillance due to her strong family history of skin cancer. Although some suspicious lesions were excised in the past, none were found to be malignant. On initial presentation at the family medicine practice, the skin was examined and no suspicious lesions were noted. In order to complete a full inspection, the patient’s gynecologist did a full anogenital examination and found no suspicious lesions. No primary site was ever located, leading to the suspicion of MUP.
DISCUSSION
Melanoma of unknown primary (MUP) is defined as a metastatic melanoma discovered first in the lymph nodes, subcutaneous tissue, or viscera without a known primary site. MUP only appears in 3.2% of patients diagnosed with melanoma [4]. Due to its rarity, it is understudied with no clear etiology, prognosis, or well-understood treatment implications for these patients.
There are three proposed hypotheses on the origin of MUP: primary tumor regression post-metastasis, a de novo melanoma, or a concurrent unrecognized melanoma versus a previously traumatically removed melanoma. MUP presents more often in males than females at a 2:1 ratio. Disease most frequently presents in the lymph nodes including the axillary, cervical, and inguinal. 2.3%-16.6% of patients with MUP present with palpable nodal disease [3]. Females present with disease most commonly in the inguinal lymph node [4] while males present with disease more commonly in the axillary lymph nodes [5].
Without significant risk factors, the current guidelines recommend observing patients with peripheral lymphadenopathy for 3-4 weeks before pursuing further workup and lymph node biopsy. However, for patients with known risk factors for malignancy, including risk factors for melanoma, workup including an ultrasound with fine needle aspiration cytology may be indicated [6]. Furthermore, once MUP is identified, a meticulous search for a primary site is necessary [7].
MUP has a slightly better prognosis than melanoma with a known primary. Prognostic factors include patient age (with a survival advantage in younger aged patients), gender, number of lymph nodes involved and distant metastatic sites involved in the disease process. Presence of extracapsular extension and an increased number of affected nodes are significantly negative prognostic factors for overall survival [8]. Treatment options include surgery to decrease tumor burden, immunotherapy, chemotherapy and radiation [7]. Though, patients who received adjuvant chemotherapy or radiotherapy had poorer survival [9]. Relapse rates, especially within 2 years of treatment, are high [7]. 56% of MUP patients had recurrence of disease and of those; majority (76%) had distant recurrences [5].
CONCLUSION
Early detection of melanoma is essential to improving prognosis, this is more difficult in patients presenting with MUP. Patients with known risk factors for melanoma who present with peripheral lymphadenopathy, as seen in this case, should be offered referral for biopsy. Upon diagnosis of MUP, a thorough search for a primary site is necessary. Currently, the most effective treatment options include surgery and immunotherapy. Still, more research is crucial to understanding this disease process in order to more effectively identify patients at risk and approach treatment options. Because of high relapse rates, patients diagnosed with and treated for MUP should be closely monitored.









































































































































{kind=link}