Breast Milk on the Infant Faecal Microbiome: Components of Breast Milk Orchestrating the Establishment of Bifidobacteria Species
- 1. Next Generation Science Institute, Morinaga Milk Industry Co., Ltd., Japan
Abstract
The initial colonization and early development of the gut microbiome during infancy are important to lifelong human health. Breast milk is the gold standard in infant nutrition. In addition to providing a source of nutrition for infants, breast milk has also been shown to play a role in the assembly of a wellbalanced and healthy infant gut microbiome, often dominated by Bifidobacterium species. Bifidobacteria are ubiquitous inhabitants of the gastrointestinal tract of mammals that are perceived as safe, beneficial microorganisms. Generally, bifidobacterial species that are commonly found in human intestines are referred to as human-residential bifidobacteria (HRB). Among HRB, infant-type HRB represent the major members of infant gut microbiota during breastfeeding period. It is increasingly evident that breast milk functions to orchestrating the establishment of bifidobacteria in infant gut. In this review, we aim to discuss about the functional role of the components in breast milk, particularly human milk oligosaccharides (HMOs) as well as the antimicrobial compounds, lysozyme, in the selection of the species of infant-type HRB as the exclusive members in infant gut microbiome.
Keywords
- Infant gut microbiota
- Infant-type humanresidential bifidobacteria
- Bifidobacterium
- Human milk oligosaccharides
- Lysozyme
Citation
Wong CB, Xiao JZ (2018) Breast Milk on the Infant Faecal Microbiome: Components of Breast Milk Orchestrating the Establishment of Bifidobacteria Species. J Hum Nutr Food Sci 6(2): 1123.
ABBREVIATIONS
HMOs: Human Milk Oligosaccharides; HRB: HumanResidential Bifidobacteria; LNB: Lacto-N-Biose; LNT: Lacto-NTetraose
INTRODUCTION
Infant gut colonization begins at birth, when the newborn is exposed to an environment full of microbes, and continues to develop during the first 2-3 years of life, until it achieves an adult-like microbial composition. The initial colonization process has an impact on several aspects of infant health, particularly in the intestinal and immunological development [1]. Improper colonization and establishment of infant gut microbiota have been intricately linked to health problems and diseases later in life [2,3].
Many lines of evidence have shown that the microbial composition of the gut microbiota in early life is greatly affected by the type of infant feeding, either breast or formula milk [4-6]. Breast-fed infants are predominantly colonized by the members of Bifidobacterium, a genus regarded as beneficial and commonly applied as probiotics. In contrary, formula-fed infants develop a more diverse microbial community with a lower proportion of bifidobacteria, while the phyla Firmicutes and Proteobacteria gain in abundance. This preponderance of bifidobacteria has led to the interest to elucidate the mechanisms by which breast milk influences the microbiota, particularly the establishment of bifidobacteria in infant gut.
Human breast milk is a rich source of nutrients and energy that promotes survival and healthy development of the newborn [7]. Accumulating evidence suggests a substantial role of breast milk bioactive molecules, especially human milk oligosaccharides (HMOs) in shaping the infant gut microbiome. HMOs are the third most abundant component in breast milk. They are indigestible by intestinal enzymes, and thus can reach the infant colon and serve as selective factor preventing the colonization of pathogenic bacteria and nurturing the growth of beneficial bifidobacterial species in infant gut [8]. In addition, breast milk also contains a myriad of antimicrobial compounds such as lysozyme, lactoferrin, immunoglobulins, and lactoperoxidase that are possibly involved in the formation of infant gut microbiota [9,10].
In this review, we aim to provide an insight regarding how human breast milk influences the development of the infant gut microbiome. Here, we will address the strategies associated with the compatibility of infant-type human-residential bifidobacteria (HRB) in human breast milk; with an emphasis on HMOs and lysozyme as the primary bifidogenic components of human breast milk in orchestrating the colonization of bifidobacteria in the infant gut.
Ecology of Bifidobacteria
Bifidobacteria naturally inhabit a range of ecological niches [11]. In humans, bifidobacteria are considered a predominant bacterial group in the infant gut microbiome and continued to be one of the most numerous bacteria during adulthood, although the numbers of bifidobacteria in guts drastically decrease with age [12]. In general, bifidobacteria could be categorized into two major groups; bifidobacterial species of human origins as humanresidential bifidobacteria (HRB) while other species which are the natural inhabitants of animals or environment as non-HRB (Figure A) [10].
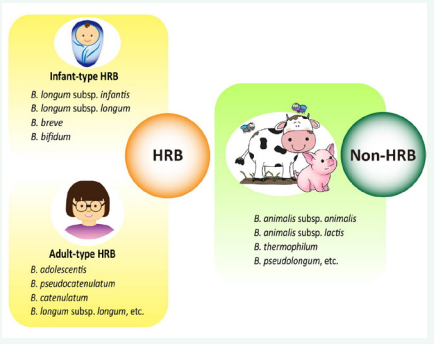
Figure A
Among HRB, four bifidobacterial species that are commonly found in the infant intestine, namely B. longum subsp. infantis, B. longum subsp. longum, B. breve, and B. bifidum, are grouped as infant-type HRB [13], while other species, including B. adolescentis, B. pseudocatenulatum, B. catenulatum, B. longum subsp. longum, etc., that are frequently isolated from the adult intestine are grouped as adult-type HRB [14]. Thereafter, B. longum subsp. longum was referred to the species that dominant in both of the infant and adult intestines [15]. Of note, infant-type HRB are the exclusive members of the gut microbiota of breastfed infants [16,17] while several species of adult-type HRB such as B. adolescentis and B. pseudocatenulatum have also been found in the faeces from formula-fed infants [18]. In view of the ecological distribution of bifidobacterial species, it is plausible that the nonessential components in human breast milk, particularly HMOs, have a significant impact on the infant gut microbiota.
Figure A. Ecological distribution of the prominent species of human-residential bifidobacteria (HRB) and non-humanresidential bifidobacteria (non-HRB).
Compatibility of infant-type HRB with human breast milk
Studies on the compatibility of HRB and non-HRB with human breast milk reveal a prominent feature of infant-type HRB in which these bifidobacterial species are highly compatible with human breast milk [19,20]. For instance, a recent in vitro study demonstrated that, among the infant-type HRB studied, all strains of B. breve and B. longum subsp. infantis were able to grow well in breast milk, while the compatibilities of B. longum subsp. longum and B. bifidum with breast milk appeared to be straindependent [19]. In contrast, most strains of adult-type HRB and non-HRB failed to grow in breast milk wherein their viable cell numbers were drastically decreased after incubation in breast milk as compared to the inoculated cell numbers [19]. Therefore, it is plausible that the bioactive components that are present in the breast milk act as selective factors for infant-type HRB, thereby contributing to their colonization in infant gut
Utilization of Human Milk Oligosaccharides (HMOs)
HMOs have been extensively studied as the primary bifidogenic components of human breast milk, owing to their structural uniqueness that can selectively promote the growth of bifidobacteria [21,22]. HMOs compose of a lactose core that are elongated by the repeats of β-1,3- or β-1,6-linked lacto-N-biose (LNB) or N-acetyllactosamine, and can be further decorated by fucose and/or sialic acid residues [23,24]. To date, over 200 different molecular structures of HMOs have been identified and among them, four HMOs, namely lacto-N-tetraose (LNT), lacto-Nfucopentaose I (LNFP I), lacto-N-difucohexaose I (LNDFH I), and 2’-fucosyllactose are over abundantly found in human breast milk [25]. It is noteworthy that three of the four predominant HMOs are type 1 chain oligosaccharides that contain LNT structure, suggesting that degradation of the type I HMO central moiety, LNT, and its constituent component, LNB could be an important step in HMOs metabolism.
Bifidobacteria produce various kinds of glycosidase enzymes for the metabolism of diverse carbohydrates in the gut. Nevertheless, not all bifidobacterial species can utilize HMOs. It is evident that, based on the residential origins, different species of bifidobacteria possess different degree of degradation and preferences in HMOs consumption [10]. In fact, HMOs consumption is a specific characteristic of infant-type HRB, whereas other species dominant in the adult gut or animals (adult-type HRB and non-HRB) are capable of fermenting complex carbohydrates but not HMOs [26]. Of the species of infant-type HRB, B. longum subsp. infantis, which is regarded as the champion colonizer of infant gut, devotes a significant portion of its genomes to the metabolism of HMOs [27]. The possession of a large cassette of HMOs degradation-related genes enables it to simultaneously utilize distinct classes of HMOs as the sole carbon source and grow vigorously with higher cell densities than other infant-type HRB that are only able to partially consume HMOs [28,29].
In general, B. longum subsp. infantis imports a variety of intact HMOs, preferably small HMOs, and hydrolyses these HMOs with intracellular glycoside hydrolases into monosaccharides for ATP production [30]. In contrast, the other species of infant-type HRB, B. bifidum sequentially consumes HMOs with an extracellular process [31] while B. longum subsp. longum and B. breve seems to exhibit partial compatibility with HMOs and grow modestly on pooled HMOs [28,32]. They degrade solely LNT, leaving other intact HMOs unmodified [33,34]. The different degradation degrees and pathways of infant-type HRB were recently reviews in detail [10]. Taken together, these studies underline the unique compatibility of infant-type HRB with human breast milk and explain their competency in the infant host. The findings have provided proof of concept on the role of human breast milk in shaping the infant gut microbiome and promoting healthy infant development.
Tolerance to lysozyme
It is noteworthy that, since human breast milk also contains an essential amount of lactose (approximately 7.0 mg/ml) that can support the growth of bifidobacteria [35], it seems that HMOs might not be the sole component that contributes to the growth inhibition of non-HMOs-utilizing adult-type HRB and non-HRB in breast milk. For this reason, it is therefore not exaggerated to consider the antimicrobial compounds, particularly human milk lysozyme, as a selective factor for infant-type HRB in infant gut. It is increasingly evident that human milk lysozyme may affect the composition of bifidobacterial species dominating in infant’s gut [19,20,36]. Lysozyme is one of the main antimicrobial factors that present abundantly (up to 400 µg/ml) in human breast milk, which is approximately 3000-fold higher than those in the bovine milk [37]. It is a bacteriolytic enzyme that catalyses the cleavage of the glycosidic linkage in bacterial peptidoglycan cell wall [38]. Recent studies have revealed that most infanttype HRB strains exhibited tolerance to high concentrations of lysozyme, while adult-type HRB strains displayed intermediate tolerance, and non-HRB strains were susceptible to both human and egg white lysozymes [19,20,39]. It is worth noting that the lysozyme tolerance of infant-type HRB is positively correlated with their capabilities to grow in breast milk [19], suggesting human milk lysozyme could also contribute to the stimulation of infant-type HRB in infant gut. In addition, it was reported that the mechanism of the lysozyme tolerance of infant-type HRB is likely to be associated with their tolerance to the cationic property of lysozymes [40]. Furthermore, one study comparing the compositions of faecal microbiotas of human breast milk fedor formula-fed infants evidenced that HMOs and lysozyme, which are typically found in human breast milk but not infant formulas, could influence the abundancy of infant-type HRB in infant faecal microbiota [41]. Together, these findings indicate that lysozyme tolerance as well as HMOs utilization could be the strategies associated with the compatibility of infant-type HRB in human breast milk.
CONCLUSIONS
The impact of breast milk on the infant gut microbiota is intriguing and still far from being understood. Breastfeeding has been associated with the dominance of bifidobacteria in infant gut microbiota, demonstrating the presence of milk components as selective colonization factors. This short review highlights that HMOs as well as lysozyme are the key determinants of the establishment of infant-type HRB as the exclusive members of the infant gut microbiome (Figure B).

Figure B
Infant-type HRB are highly compatible with human breast milk for which they are differentially equipped with an arsenal of HMOs-degrading enzymes to utilize HMOs as a carbon source and are highly tolerant to lysozyme. Current research on the molecular mechanisms of HMOs utilization provides insights into the impact of breast milk on infant gut microbiome and underscores the necessity of breastfeeding as the first source of nutrition.
(Figure B) Schematic overview of the key determinants in human breast milk that contribute to the colonization of infanttype HRB as the exclusive members of the infant gut microbiome. HMOs and lysozyme act as the primary bifidogenic components of human breast milk that selectively promote the colonization of infant-type HRB in infant gut. Infant-type HRB are capable of utilizing HMOs as a carbon source and possess high tolerance to lysozyme.
REFERENCES
7. Oftedal OT. The evolution of milk secretion and its ancient origins. Animal. 2012; 6: 355-368.
11. Biavati B, Mattarelli P. The family bifidobacteriaceae. The prokaryotes: Springer. 2006; 322-382
21. Marcobal A, Barboza M, Froehlich JW, Block DE, German JB, Lebrilla CB, et al. Consumption of human milk oligosaccharides by gut-related microbes. J Agric Food Chem. 2010; 58: 5334-5340.
36. Sugahara H, Odamaki T, Xiao J. Genotypic and Phenotypic Evaluation Revealed the Appropriateness of Human-Residential Bifidobacteria for Human Use Milk science. 2015; 64: 261-269.
38. Jollès P, Jollès J. What’s new in lysozyme research? Always a model system, today as yesterday. Mol Cell Biochem. 1984; 63: 165-189.








































































































































