Compliance with National Operational Guidelines for Community Management of Acute Malnutrition among Community Health Workers in Konduga Local Government Area of Borno State, Nigeria
- 1. Department of Epidemiology and Medical Statistics, University of Ibadan, Nigeria
- 2. Department of Animal Production and Health, Federal University of Technology Akure, Nigeria
- 3. Department of Surgery, Federal Medical Center, Keffi, Nigeri
Abstract
Background: Community Management of Acute Malnutrition (CMAM) is a proven approach for the reduction of under-five morbidity and mortality in Nigeria.
Objective: To assess knowledge of and compliance with National Operational Guidelines (NOG) for Community Management of Acute Malnutrition (CMAM) among Community Health Workers (CHWs).
Method: A descriptive cross-sectional study was conducted in Primary Health Care (PHC) facilities in Konduga Local Government Area of Borno State, Nigeria. All 48 CHWs providing CMAM services were included in the study, and assessed on knowledge and compliance with NOG for CMAM. A point was assigned to correct response to 6 knowledge and 5 compliance questions. Respondents with scores above 3 were categorized as those with good knowledge, while those with scores above 2 were categorized as good compliance. Data were analyzed using independent samples T-test and correlation analysis, with the level of significance set at 0.05.
Results: Generally, 29 (69.0%) of the respondents had good knowledge of the CMAM guidelines, and 31 (73.9%) had good compliance with the guidelines. High level of compliance with the CMAM guidelines was significantly associated with having 5 or more years of working experience (t (30.6) = -2.27, P = 0.030) and increase in the level of knowledge of the guidelines (r = 0.37, P = 0.017).
Conclusion: Our findings revealed that the level of compliance with the CMAM guidelines is high particularly among health workers with high years of working experience and high level of knowledge of the CMAM guidelines. Regular training of health workers on the guidelines, particularly among those with low years of experience is recommended.
Keywords
• Community management of acute malnutrition
• National operational guidelines
• under-five children
• Community health workers
Citation
Adejugbagbe AM, Ajayi IOO, Ayegbusi AO, Oki OP (2020) Compliance with National Operational Guidelines for Community Management of Acute Malnutrition among Community Health Workers in Konduga Local Government Area of Borno State, Nigeria. J Hum Nutr Food Sci 8(2): 1135.
INTRODUCTION
The term malnutrition among children generally refers to under-nutrition including protein-energy malnutrition and deficiency of micronutrients. Under-nutrition such as stunting is declining too slowly while wasting still impacts the lives of far too many young children [1]. Globally in 2018, an estimate of 49.5 million (7.3%) of under 5 children were wasted and 149 million (21.9%) were stunted. In the same year, 55% and 68% of all stunted and wasted under-5 children lived in Asia, while 39% (stunted) and 28% (wasted) lived in Africa [1]. In West Africa, 29% of under-5 children were estimated to be malnourished, and Nigeria accounted for 22% and 37% of underweight and stunted among under-5 children respectively. Among the six geopolitical zones in Nigeria, the highest prevalence of stunting (57%) was found in the North West region followed by North east with a prevalence of 49% [2].
Community Management of Acute Malnutrition (CMAM) is a proven approach to manage Severe Acute Malnutrition (SAM) and Moderate Acute Malnutrition (MAM) among under-5 children in more than 70 countries [3]. This approach involves early detection of SAM children by community volunteers and treatment with Ready-to Use Therapeutic Food (RUTF) or other nutrient-dense foods at home. The CMAM approach is divided into four components that include; community mobilization to raise awareness and ensure community involvement, Outpatient Therapeutic Programme (OTP) for the management of SAM without medical complications, Stabilization Care (SC) for hospital-based management of complicated SAM case and supplementary feeding programmes for management of MAM through nutrition care.
Nigeria had developed National Operational Guidelines (NOG) and training manuals for CMAM with emphasis on management of severe malnutrition at Primary Health Care (PHC) facilities or OTP sites, and at inpatient or Stabilization Care (SC) center [4]. According to WHO (2013), the use of NOG for CMAM in the management of SAM had contributed immensely to the reduction of case fatality load in the facilities and strengthened the effective and safe nutrition actions to counteract the public health effects of malnutrition [5]. The guidelines for CMAM were developed taking into consideration Nigeria’s localities and circumstances, and seek to provide practical guide to health and nutrition workers who design, implement, monitor and evaluate acute malnutrition management programmes at all level of the facilities [4].
In Nigeria, outpatient treatment of SAM are delivered by trained health workers from primary health care facilities, however, some major constraints have been reported among them in different countries [6,7]. For instance, inability to provide the recommended amount of RUTF and inappropriate exit of admitted children from the OTP site were reported in earlier studies in Pakistan and Ethiopia where the CMAM program is being implemented [6,7]. According to our literature search, no published study had investigated compliance with CMAM guidelines particularly among the nutrition services providers in Nigeria. Examining service delivery in accordance with the national guidelines has the potential to identify constraints for achieving acceptable program performance. This study aim to explore knowledge of and compliance with NOG for CMAM among Community Health Workers (CHWs) in government health facilities in Konduga LGA, Borno State.
MATERIALS AND METHODS
Study area
The study was conducted in Konduga Local Government Area (LGA), Borno State located in the North East zone of Nigeria. Borno state was formed in 1976 with the capital in Maiduguri. Konduga LGA is one of the 27 Local Government Areas (LGAs) of the state, and located in the Central Senatorial District. The LGA has an area kilometer of 6,065.89 km2 and a population of 233,736 in 2018, projected from the 2006 census population [8]. The primary languages of the population in the LGA are Hausa, Shuwa, Arabic, Kanuri and Wandala/Malgwa.
Konduga LGA was divided into a total of 11 wards, in which 7 were accessible in 2018. Twenty-five (25) government Primary Health Care (PHC) facilities were available in the 11 wards of the LGA to provide essential PHC services in 2018. Among the accessible wards, 4 were designated as CMAM implementing sites with 12 OTP sites available in these wards. Seven of the OTP sites were located in PHC facility in the community, 3 were located in Internally Displaced Persons (IDP) camps and 2 were located in outreach sites. A total of 4 CHWs were designated to provide CMAM services in each OTP site.
Study design and participants
A descriptive cross-sectional study was conducted between January and February 2018. The study participants were CHWs providing CMAM services in communities and IDP camps. All CHWs providing CMAM services were included in the study, while health workers that were ill or not available during the period of the study were excluded.
Data collection, management and analysis
Data were obtained using a piloted semi-structured, selfadministered questionnaire. Data on respondents’ sociodemographic characteristics, work history, knowledge and compliance with NOG for CMAM were included in the questionnaire. The questions were entered into data collection software called Kobo Toolbox that was installed on mobile phone, and used to obtain data from the respondents. Knowledge of respondents on guidelines for CMAM was assessed with 6 itemized questions, while compliance with the guidelines was determined using 5 questions. A point was assigned to correct response to each question, respondents with knowledge score above 3 were categorized as those with good knowledge, and those with compliance score above 2 were considered as those with good compliance with the NOG for CMAM.
Data management and analysis
Data were analyzed with Statistical Package for the Social Sciences (SPSS) version 20 software. Frequency tables and graphs were generated. The independent variables including socio-demographic characteristics, working experience and knowledge of NOG for CMAM were analyzed with the dependent or outcome variable being compliance with the CMAM guidelines. Independent samples t-test and correlation analysis were used to identify factors associated with compliance with the guidelines. The relationship between knowledge of and compliance with NOG for CMAM was determined using correlation analysis. P-value was obtained and the level of significance was set at 0.05.
Ethical approval
Ethical approval for the study was obtained from the Ethical Review Committee of the Borno State Ministry of Health. Written informed consent was obtained from the participants before the interview was conducted. Confidentiality of data obtained was ensured by identifying the questionnaires with numbers instead of names, and every data obtained was safely locked and protected from third party.
RESULTS
Socio-demographic characteristics of respondents
A total of 42 respondents were interviewed among the 48 Community Health Workers in the Outpatient Therapeutic Program sites in the LGA, with a response rate of 87.5% achieved. Half (21; 50.0%) of the respondents were above 35 years of age (range: between 24 and 54 years). Majority (28; 66.7%) of them were females and 27 (64.3%) were married (Table 1).
|
Table 1: Socio-demographic characteristics of respondents (N=42). |
||
|
|
Frequency |
Percentage |
|
Location of OTP site |
|
|
|
Health Facility |
25 |
59.5 |
|
Internally Displaced Persons camp |
11 |
26.2 |
|
Outreach |
6 |
14.3 |
|
Age (years) |
|
|
|
< 30 |
13 |
31.0 |
|
30-35 |
8 |
19.0 |
|
>35 |
21 |
50.0 |
|
Gender |
|
|
|
Male |
14 |
33.3 |
|
Female |
28 |
66.7 |
|
Marital Status |
|
|
|
Single |
12 |
28.6 |
|
Married |
27 |
64.3 |
|
Widow |
3 |
7.1 |
|
Ethnic group |
|
|
|
Kanuri |
20 |
47.6 |
|
Bura |
10 |
23.8 |
|
Hausa |
3 |
7.1 |
|
Fulani |
1 |
2.5 |
|
*Others |
8 |
19.0 |
|
Religion |
|
|
|
Islam |
29 |
69.0 |
|
Christian |
13 |
31.0 |
|
Current position |
|
|
|
CHEW |
19 |
45.2 |
|
+Others |
13 |
31.0 |
|
Nurse/Midwife |
7 |
16.7 |
|
Health Assistant |
3 |
7.1 |
|
Type of Job |
|
|
|
Government full time job |
13 |
31.0 |
|
Contract |
26 |
61.9 |
|
Volunteer |
3 |
7.1 |
|
Highest level of education |
|
|
|
Tertiary |
38 |
90.5 |
|
Post tertiary |
4 |
9.5 |
|
Monthly income in Naira |
|
|
|
≤50,000 |
33 |
78.6 |
|
>50,000 |
9 |
21.4 |
|
*others= Marghi, Shuwa, Glavda; +Biology Education, Environmental Health Officer, Laboratory Technician. CHEW: Community Health Extension Worker; OTP= Outpatient Therapeutic Program |
||
Nineteen (45.2%) of the respondents were Community Health Extension Workers (CHEW) followed by other professions such as Environmental Health Officers and Laboratory Technicians (13; 31.0%).
Working experience and CMAM training received among respondents
Table 2 below shows that 19 (45.2%) of the respondents were yet to have 5 months working experience in CMAM program. Majority 39 (92.9%) of them reported to have been trained on CMAM, while 36 (92.3%) among those trained reported to have received training in the last 1 year. More than a quarter (13; 33.3%) of the respondents received training once since they have been providing CMAM services.
|
Table 2: Working experience and CMAM training received among respondents (N=42). |
||
|
Frequency |
Percentage |
|
|
Months of working experience as CMAM provider |
||
|
< 5 months |
19 |
45.2 |
|
5- 20 months |
9 |
21.6 |
|
>20 months |
14 |
33.2 |
|
Ever been trained on CMAM |
||
|
Yes |
39 |
92.9 |
|
No |
3 |
7.1 |
|
When CMAM training was received last (N=39) |
||
|
In the previous 1 year |
36 |
92.3 |
|
In the previous 2 years |
3 |
7.7 |
|
Number of times trained on CMAM (N=39) |
||
|
1 |
13 |
33.3 |
|
2 |
9 |
23.1 |
|
3 |
8 |
20.5 |
|
> 3 |
9 |
23.1 |
|
CMAM= Community Management of Acute Malnutrition |
||
Knowledge of National Operational Guidelines for Community Management of Acute Malnutrition among respondents
Table 3 shows knowledge of respondents about NOG for CMAM. Eighteen (42.9%) of the respondents knew that a child should pass appetite test before being admitted.
|
Table 3: Knowledge of National Operational Guidelines for Community Management of Acute Malnutrition among respondents (N=42). |
||
|
|
Frequency |
Percentage |
|
A child is admitted into CMAM program if he or she meet any of the following criteria |
|
|
|
+MUAC measurement is equal to 11.5 |
19 |
45.2 |
|
Presence of medical complications |
2 |
4.8 |
|
Ability of the child to pass appetite test |
18 |
42.9 |
|
Don’t know |
3 |
7.1 |
|
A child is discharged as cured if he or she meet any of the following criteria |
|
|
|
MUAC measurement is equal to 12.5cm for 2 consecutive visits |
17 |
40.5 |
|
Reduction in child weight |
1 |
2.4 |
|
MUAC measurement is greater than 12.5cm for 2 consecutive visits |
23 |
54.7 |
|
Don’t know |
1 |
2.4 |
|
A defaulter is a child that was absent for how many visits in programme |
|
|
|
One visit |
5 |
11.9 |
|
Two consecutive visits |
2 |
4.8 |
|
Three consecutive visits |
35 |
83.3 |
|
A child with generalized oedema (+++) can be admitted at the OTP site |
|
|
|
Yes |
7 |
16.7 |
|
No |
35 |
83.3 |
|
Don’t know |
|
|
|
Antibiotic such as amoxicillin can be given only during second visit of patient to the OTP site |
|
|
|
Yes |
7 |
16.7 |
|
No |
35 |
83.3 |
|
Albendazole can be given to a child that is less than a year |
|
|
|
Yes |
11 |
26.2 |
|
No |
30 |
71.4 |
|
Don’t know |
1 |
2.4 |
|
Mean knowledge score (standard deviation) |
4.2±1.51 |
|
|
+ MUAC= Mid Upper Arm Circumference; CMAM= Community Management of Acute Malnutrition |
||
Slightly above half (23; 54.8%) of the respondents knew that MUAC measurement of child should be above 12.5cm for 2 consecutive visits as one of the discharge criteria. In general, 29 (69%) of the respondents had good knowledge of the NOG for CMAM, with mean knowledge score of 4.2±1.51.
Availability of National Operational Guidelines for Community Management of Acute Malnutrition among respondents
About two-third [26 (62%)] of the respondents had a copy of the NOG for CMAM. Among those having the guidelines, 13 (50.0%) reported to have referred to it for clarification in the last one week preceding the study (Figure 1).
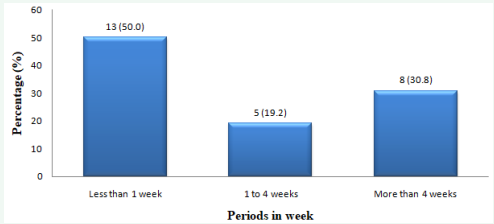
Figure 1: Periods respondents last referred to the National Operational Guidelines for CMAM for clarifications.
Compliance with National Operational Guidelines for CMAM among respondents
In Table 4, 24 (57.1%) of the respondents replied that they conduct appetite test before enrolling children into CMAM program.
|
Table 4: Compliance with National Operational Guidelines for CMAM among respondents (N= 42). |
||
|
Frequency |
Percentage |
|
|
Which of these is used to assess admission of child into CMAM program |
||
|
Appetites test |
24 |
57.1 |
|
Child weight measurement |
6 |
14.3 |
|
Document on the admission card |
5 |
11.9 |
|
Don’t know |
5 |
11.9 |
|
Give weekly ration of RUTF to caregiver of patient |
2 |
4.8 |
|
Action taken whenever a SAM case with medical complications is found during OTP session |
||
|
Refer to stabilization center |
30 |
71.4 |
|
Continue treatment in the OTP |
5 |
11.9 |
|
Give medication to the child in the OTP |
5 |
11.9 |
|
Conduct outpatient consultation for the SAM case at the OTP site/HF |
2 |
4.8 |
|
Action taken whenever a SAM case misses three consecutive visits and return to the OTP site |
||
|
Continue treatment on a new admission card only if he or she meet the admission criteria |
33 |
78.6 |
|
Continue treatment on the same admission card |
9 |
21.4 |
|
Action taken whenever a patient has MUAC measurement of 11.5cm after 12 consecutive weeks in the program |
||
|
Refer to stabilization center |
25 |
59.5 |
|
Refer to inpatients in the hospital |
9 |
21.4 |
|
Report to supervisors |
4 |
9.5 |
|
Conduct no action |
2 |
4.8 |
|
*Others |
2 |
4.8 |
|
Action taken whenever a patient presented with SAM after two months of discharge from the OTP site |
||
|
Consider child as a new SAM case and admit using a new admission card |
33 |
78.6 |
|
Refer to the stabilization center |
4 |
7.1 |
|
Provide IYCF counseling to the caregiver of child only |
1 |
2.4 |
|
Don’t know |
5 |
11.9 |
|
*Discharge patient only, Admit the child into the program; OTP= Outpatient Therapeutic Program, SAM= Severe Acute Malnutrition; MUAC= Mid Upper Arm Circumference; CMAM= Community Management of Acute Malnutrition |
||
Whenever a SAM case with medical complication is found at the OTP site, 30 (71.4%) of the respondents said that they refer such case to the stabilization center. Overall, 31 (73.8%) of the respondents had good compliance with the NOG for CMAM.
Factors influencing compliance with National Operational Guidelines for CMAM among respondents
In Table 5, years of working experience and knowledge of NOG for CMAM were the main factors significantly related with compliance with NOG for CMAM among the respondents.
|
Table 5: Factors influencing compliance with National Operational Guidelines for CMAM among respondents. |
|||||
|
|
Mean± SD Compliance |
P-Value |
Df |
t |
95% Confidence Interval |
|
Age in years |
|
|
|
|
|
|
≤35 |
3.24 ± 1.0 |
0.296 |
37.817 |
1.06 |
0.304 -0.970 |
|
>35 |
2.90 ± 1.1 |
|
|
|
|
|
Gender |
|
|
|
|
|
|
Male |
3.21 ± 1.0 |
0.528 |
28.027 |
0.64 |
0.467 – 0.886 |
|
Female |
3.00 ± 1.1 |
|
|
|
|
|
Ethnic group |
|
|
|
|
|
|
Kanuri |
3.05 ± 1.2 |
0.899 |
34.499 |
- 0.13 |
0.687- 0.605 |
|
Other tribes |
3.09 ± 0.87 |
|
|
|
|
|
Current position |
|
|
|
|
|
|
Clinicians |
2.85 ± 1.2 |
0.068 |
39.579 |
-1.88 |
1.228 – 0.045 |
|
Non clinicians |
3.44 ± 0.6 |
|
|
|
|
|
Type of Job |
|
|
|
|
|
|
Government Paid Job |
3.00 ±1.2 |
0.766 |
20.042 |
-0.30 |
0.800-0.593 |
|
Non-government paid job |
3.10 ±1.0 |
|
|
|
|
|
Monthly income in naira |
|
|
|
|
|
|
≤50,000 |
3.12 ± 1.0 |
0.552 |
12.436 |
0.60 |
0.550- 1.015 |
|
>50000 |
2.89 ± 1.1 |
|
|
|
|
|
Working experience in years |
|
|
|
|
|
|
≤ 5 years |
2.68 ± 1.2 |
0.030 |
30.600 |
-2.27 |
-1.343- -1.000 |
|
>5 years |
3.40 ± 0.8 |
|
|
|
|
|
Have national CMAM guidelines |
|
|
|
|
|
|
Yes |
3.08 ± 1.0 |
0.965 |
30.799 |
0.04 |
0.650- 0.680 |
|
No |
3.06 ± 1.1 |
|
|
|
|
|
CMAM= Community Management of Acute Malnutrition. |
|||||
Respondents who have worked as CMAM provider for 5 year and more (3.40 ± 0.8 years) had higher mean compliance score compared to those that have worked for less than 5 years (2.68 ± 1.2 years) (t (30.6) = -2.27, p = 0.030) with a difference of 0.72 (95% CI, -1.343 to -1.000). A moderate positive correlation was found between knowledge of CMAM guidelines and compliance, r = 0.37, P = 0.017, with increase in knowledge level signifying increase in level of compliance with the guidelines among the respondents.
DISCUSSION
Nigeria as a developing country where resources are very limited requires high level of compliance with National Operational Guidelines for CMAM as a cost effective strategy to manage Severe Acute Malnutrition in the community. The study showed the level of community health workers compliance with the NOG for CMAM, alongside their knowledge of the guidelines and factors influencing level of compliance.
We found that the level of knowledge of the respondents about the CMAM guideline is high. This may be related to the fact that majority of the respondents have been trained on the guidelines, with almost all trained within the last one year prior to the study. The training on current guideline could upgrade the knowledge and skill of health workers to the extent that they would easily understand the basic principles and standard of practice of program and implement them consistently whenever it is essential to do so.
Similar to our finding, Esu et al. (2019) found high level of knowledge of standard precautions among healthcare workers in public hospitals Abuja, Nigeria [9]. The similarity of Esu et al., (2019) study with ours could be because majority of the respondents in our study were clinicians who are expected to have received training on clinical services compared to nonclinicians. Different from this study finding, Ndiema et al. (2018) found low level of knowledge of nutrition parameters among health workers in Kenya [10], Mogre et al. (2017) also found inadequate knowledge of malnutrition and its management among nurses in Ghana [11], and Abdulraheem et al. (2012) found that less than one-third of health workers in Borno State, Nigeria have inadequate knowledge of universal precautions [12]. In all these previous studies [10- 12], training of health workers on standard guidelines was identified as major factor to improve their knowledge.
Non-compliance with standard operational guidelines among health workers could be due to their belief that their workload is increased thus; these guidelines are difficult to accommodate due to day to day current clinical pressures [13]. However, following recurrent on-the job training provided to health workers, compliance with standard precaution has improved [14].
In our study, majority of the respondents have been trained on standard guidelines for CMAM, coupled with supportive supervision conducted among them when providing services. Also, majority of the respondents have a copy of the CMAM guidelines and refer to it when providing services. These findings suggest the reason majority of them complied with the guidelines in this study. Similar finding was reported among nurses in a tertiary institution in Kenya [10] and Uganda [15]. However, previous study in Borno State Nigeria reported low compliance with standard precautions among health workers [12]. Although both our study and that of previous study12 were conducted in the same state however, lack of investment in staff training may be linked with deficient in knowledge among the respondents in Borno State [12].
Healthcare workers’ years of experience and knowledge of the NOG for CMAM significantly influenced compliance with the guidelines. Similar to our findings, Kobe (2006) reported that conducting nutritional assessments correlated directly with knowledge scores in a study that determined the nutritional knowledge, attitudes and practices of nurses in Kenya [16]. Similar findings have also been reported by Yacin et al. (2013) in a study that assessed the nutritional knowledge of nurses in Turkey [17]. Earlier study conducted among physiotherapist in Netherlands found that their experience increased adherence to number or treatment sessions [18]. Likewise previous studies in Borno State [12] and Abuja, Nigeria [9] found that health workers with experience of ten years and above complied better with standard precautions compared to those with lesser years of experience. The experience and knowledge of the respondents may have worked in synergy to improve respondents’ level of compliance with the guidelines.
The findings from this study could have been limited by its cross-sectional design nature in which it does not establish definitive cause and effect relationships between the outcome and explanatory variables. Given that self-reported data were used, the reliability of the results might be negatively influenced to some extent because of response bias. To reduce such bias, questions were diversified, transparent and based on specific timeframe. Furthermore, since the study was conducted in a district of Borno State, it could be difficult to make generalization to other parts. Hence, future studies should consider including more LGAs in order to make generalization for the state.
CONCLUSION
Compliance with National Operational Guidelines for Community Management of Acute Malnutrition was high among the health workers in Konduga Local Government Area of Borno State. Having high years of experience and adequate knowledge of the CMAM guidelines were significantly associated with high level of compliance with the guidelines. Thus, regular training and on-the job coaching and mentoring are recommended for the health workers, particularly among those with few years of experience on nutrition activities and inadequate knowledge of the guidelines.
REFERENCES
1. UNICEF, WHO and World Bank Group. Levels and trends in child malnutrition. Key findings of the 2019 edition of the Joint Child Malnutrition Estimates. Geneva: World Health Organization; Licence: CC BY-NC-SA 3.0 IGO.
2. National Population Commission (NPC) [Nigeria] and ICF International. Nigeria Demographic and Health Survey. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International. 2019; 257- 296.
3. United Nations Children’s Fund. Global Evaluation of Community Management of Acute Malnutrition (CMAM): Global Synthesis Report (link is external). New York: UNICEF. 2013; 4.
4. Federal Ministry of Health, Nigeria. Family Health Department Nutrition Division. National Guidelines for Inpatient Management of Severe Acute Malnutrition in Infants and Young Children in Nigeria. 2016.
5. World Health Organization. Guideline: Updates on the management of severe acute malnutrition in infants and children. Geneva, World Health Organization 2013; 1-2.
8. City population. Borno State in Nigeria.
15. Nekatebeb HMA, Kappos K, Pomeroy A, Kyenkya M, DeAgostino A, Wamuyu, MG. Report on findings from an assessment of nutrition assessment, counseling, and support (NACS) services in Southwestern Uganda 2013. Washington DC: USAID/Strengthening Partnerships, Results and Innovations in Nutrition Globally (SPRING) Project 2013. 17-20.
16. Kobe JA. Aspects of nutritional knowledge, attitudes and practices of nurses working at the surgical division at the Kenyatta National Hospital, Kenya, University of Stellenbosch, Stellenbosch. 2006.








































































































































