No Association between Vitamin D and Physical Fitness in Trained Youth Soccer Athletes
- 1. Dakota State University, USA
- 2. Avera Sports, USA
- 3. South Dakota State University, USA
Abstract
Vitamin D is known to affect bone health and muscle function. Insufficient vitamin D (25(OH)D) status may negatively affect adolescent physical performance levels. The purpose was to examine the cross-sectional association between 25(OH)D status and several markers of physical performance in youth club soccer athletes. 42 adolescent, male and female club soccer players age 14-18 were recruited during the winter season. 25(OH)D status, measured in January, was assessed from a capillary blood sample analyzed using liquid chromatography-tandem mass spectrometry. Physical performance was evaluated using a variety of agility, muscular strength, and cardiorespiratory fitness tests. Participants were classified as 25(OH)D Deficient (< 50 nmol/L), Insufficient (50-75 nmol/L), or Sufficient (> 75 nmol/L) and a relationship between physical performance and 25(OH)D classification was determined using a one-way ANOVA. Mean 25(OH) D status was 67.0 ± 16.7 nmol/L. 19% (8/42) of the participants were vitamin D deficient, 55% (23/42) were vitamin D insufficient, and 26% (11/42) were vitamin D sufficient. There were no associations found between 25(OH)D status and the variety of agility, muscular strength, and cardiorespiratory fitness tests (P > 0.05). This investigation demonstrates there are no associations between 25(OH)D status and physical performance in adolescent soccer players. Our participants were competitive adolescent athletes with none being severely deficient which may mask associations in this population group.
KEYWORDS
- Vitamin
- Deficiency
- Athlete
- Performance
- Nutrition
CITATION
Scholten SD, Ferley DD, Vukovich MD (2024) No Association between Vitamin D and Physical Fitness in Trained Youth Soccer Athletes. J Hum Nutr Food Sci 12(3): 1190.
INTRODUCTION
Interest in 25(OH)D status has increased recently due to reports indicating that impaired physical fitness, specifically in athletes, may be associated with suboptimal 25(OH)D status [1- 5]. 57-91% of athletes are reported to have insufficient 25(OH)D status (<75 nmol/L) [6-9]. Suboptimal 25(OH)D status is likely a result from inadequate sun exposure which affects athletes who live in far southern or northern latitudes, have dark skin, train indoors, and/or train early or late in the day [10].
Suboptimal 25(OH)D status may negatively affect muscle tissue because it is associated with decreased amino acid uptake, prolonged time to peak muscle contraction and relaxation, myofibril repair, dysregulation of intracellular Ca2+, delayed muscle recovery, and impaired muscle hypertrophy [10-14]. A few researchers have suggested a 25(OH)D status to exceed 75 nmol/L [15,16], while others recommend 25(OH)D levels between 100 nmol/L and 250 nmol/L for optimal physical performance [17-19], Several authors studied the association of 25(OH)D status with physical performance, but results have been inconclusive [20,21].
Understanding that adolescent athletes have similar 25(OH)D status as adult athletes with the majority classified as insufficient [22-26], it is important to know if 25(OH)D status is associated with physical performance in this group. Insufficient 25(OH) D may negatively affect physical performance as skeletal and cardiac muscle may be influenced by 25(OH)D through many possible biological targets. The relationship between 25(OH)D status and physical fitness in youth athletes is not well understood. Therefore, we examined the cross-sectional association between 25(OH)D status and several markers of physical performance in youth club soccer athletes. We hypothesized a positive correlation between 25(OH)D status and markers of physical performance in adolescent athletes.
METHODS
Participants
42 male and female adolescent (14-18 yr) club soccer players were evaluated for 25(OH)D status during the months of January and February in Sioux Falls, SD, USA, (Latitude and longitude 43.536388, -96.731667). Before testing, verbal explanation of the aim of the study and the testing procedures were given to all participants, and written informed consent was obtained from the athletes and their parents/guardian. For individuals younger than 18 years, a child’s consent document was provided along with an informed consent document by the parent or legal guardian. We excluded individuals <13 and >18 years of age and those who had experienced a lower-body injury in the previous 3 months. This study was approved by the Avera McKennan Hospital and University Health Center’s Institutional Review Board and it conformed to the recommendations of the 1964 Declaration of Helsinki. Informed consent was obtained from all subjects involved in the study.
25(OH) D Analysis
A capillary blood sample was collected from each athlete, appropriately packaged, and sent to ZRT Laboratory (Beaverton, Oregon, USA) for 25(OH)D (D2 and D3) analysis. ZRT Laboratory participates in the Vitamin D External Quality Assessment Scheme (DEQAS). Thresholds used to indicate deficiency, insufficiency, and sufficiency were <50 nmol/L, 50-75 nmol/L, and >75 nmol/L respectively.
Performance Tests
Five to 7 days after completing familiarization testing, participants were scheduled for performance testing over 3 sessions spaced 48-72 hours apart. Participants were instructed to avoid caffeine prior to testing and were encouraged to refrain from vigorous physical activity 48 hours prior to testing. Testing order occurred as described in Figure 1.
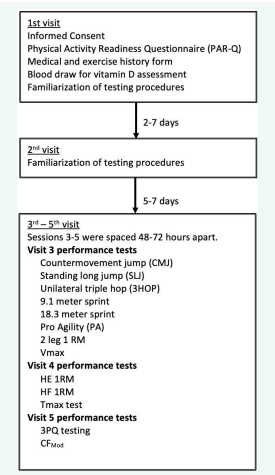
Figure 1: Study flowchart and CONSORT diagram of enrolled participants.
Testing procedures follow.
A brief description of each performance test follows as detailed descriptions were provided in an earlier publication [27].
Counter Movement Jump (CMJ)
A VERTEC (Questtek Corp., Northridge, CA, USA) was used to asses jump height using the best attempt over three trials.
Unilateral triple hop (3HOP)
This tests assesses the maximum jump distance of three consecutive hops using the same leg. The best of 3 trials was used for data analysis.
9.1 & 18.3 m sprints (10 & 20 yard)
An infrared timing system (Brower Timing Systems, Draper, UT, USA) was used to assess sprint speed from a three-point stance over a 9.1 m and 18.3 m distance on an indoor track surface.
Pro Agility (PA)
Participants began in a 3-point stance and sprinted as fast as possible to a marker 4.6 m away, rotated 180 degrees to run to the next marker 9.1 m away, returning to the start line. The best of three trials was recorded.
PlyoPress 2 leg strength (2 leg-1RM)
A PlyoPress (Plyo Press 625 III, Frappier Acceleration, Fargo, ND) was used to assess lower leg strength. This assessment is similar to a traditional squat but in the supine position. Resistance increased until a 1-RM was determined.
Vmax
A Super Treadmill (Standard Industries, Fargo, ND, USA) set at 1.0% incline was used to assess maximum velocity a participant could maintain for a minimum of 90 seconds. Speed increased by 0.80 km/hr for each 2-minute stage. The speed of the last completed stage was defined as the Vmax [28].
Hip flexion/extension strength (HF-1RM, HE-1RM)
A Pro Multi-Hip (Standard Industries, Fargo, ND, USA) was used to determine maximal hip flexion and extension strength on each participant’s dominant lower limb. 1-RM efforts were attempted until failure.
Tmax
Participants completed the Tmax test using proceedures from previous research [29]. Participants ran at their VO2max velocity until a maximum voluntary time effort.
Plyo Press Power Quotient (3PQ)
Participants explosively jumped continuously for 30 seconds on a Plyo Press (Plyo Press 625 III, Frappier Acceleration, Fargo, ND). Power from the force platform was recorded for the duration.
Cunningham/Faulkner modified (CFMod)
This test required participants to run to voluntary exhaustion at their VO2max velocity on a Super Treadmill (Standard Industries, Fargo, ND, USA) set to 20% incline.
Statistical Analysis
The statistical analysis program JMP (v.13.0, SAS Institute, Cary, NC, USA) was used for all data analysis. Descriptive statistics of each outcome variable, including means, standard deviations were determined. One-way analysis of variance (ANOVA) was used to compare performance measure means and variances between three levels of 25(OH)D status, <50 nmol/L, 50-75 nmol/L, and >75 nmol/L. A p-value <0.05 was considered cut-off for statistical significance.
RESULTS
42 youth soccer participants completed the vitamin D assessment and all performance measures. Participant characteristics are presented in Table 1.
Table 1: Athlete characteristics.
|
|
Mean (SD) |
Min-max |
|
Age |
15.7 (1.1) |
14-18 |
|
Height (cm) |
167.1 (8.6) |
60.0-72.5 |
|
Weight (kg) |
62.7 (11.5) |
86.0-195.0 |
|
BMI (kg/m2) |
22.3 (3.3) |
16.3-30.1 |
All data was collected from January to February. Participants were excluded if they had a current or recent injury which prevented them from performing any of the testing protocol. Data collection was performed in Sioux Falls, SD (latitude 43.5ºN).
The mean 25(OH)D status in this study population was 67.0 ± 16.7 nmol/L. 19% (8/42) of the participants were vitamin D deficient, 55% (23/42) were vitamin D insufficient, and 26% (11/42) were vitamin D sufficient. Mean 25(OH)D status was similar between males and females (67.7 ± 17.4 nmol/L vs 65.5 ± 17.0 nmol/L, p = 0.83). No statistical significance was found in any of the physical performance tests between the vitamin D deficient, insufficient, and sufficient groups (P > 0.05) (Table 2 & 3).
Table 2: Athlete 25(OH) D concentration.
|
|
Sample size |
Mean (SD) |
Min-max |
|
Deficient (< 50 nmol/L) |
8 |
45.8 (3.75) |
39.9-49.9 |
|
Insufficient (50-75 nmol/L) |
23 |
63.1 (5.93) |
52.4-74.9 |
|
Sufficient (>75 nmol/L) |
11 |
90.8 (8.07) |
77.4-104.8 |
|
Overall (nmol/L) |
42 |
67.0 (16.7) |
39.9-104.8 |
Table 3: Performance results in Vitamin D Sufficient, Insufficient, and Deficient Soccer Players
|
Parameter |
Vitamin D Deficient (n=8) |
Vitamin D Insufficient (n=23) |
Vitamin D Sufficient (n=11) |
p Value |
|
CMJ (cm) |
51.1 (7.8) |
52.8 (10.4) |
54.3 (11.6) |
0.79 |
|
SLJ (m) |
1.95 (0.28) |
1.96 (0.34) |
2.10 (0.31) |
0.42 |
|
3HOP (m) |
5.04 (0.76) |
4.94 (0.85) |
5.14 (0.61) |
0.78 |
|
9.1m (sec) |
2.03 (0.09) |
1.98 (0.17) |
1.98 (0.20) |
0.71 |
|
18.3m (sec) |
3.40 (0.22) |
3.35 (0.30) |
3.31 (0.35) |
0.81 |
|
PA (sec) |
5.24 (0.19) |
5.21 (0.36) |
5.13 (0.41) |
0.77 |
|
CFMOD (sec) |
42.6 (9.57) |
40.26 (9.72) |
44.45 (10.52) |
0.5 |
|
Vmax (m/sec) |
3.91 (0.41) |
4.09 (0.40) |
4.26 (0.33) |
0.15 |
|
Tmax (sec) |
202.00(26.48) |
170.30 (55.79) |
185.90 (33.83) |
0.24 |
|
2 Leg-1RM (kg) |
131.24(29.92) |
129.66 (32.11) |
137.31 (36.27) |
0.81 |
|
HE-1RM (kg) |
69.17 (14.64) |
64.58 (16.76) |
71.12 (11.02) |
0.46 |
|
HF-1RM (kg) |
47.90 (12.20) |
47.13 (11.53) |
52.78 (10.68) |
0.4 |
|
3 PQ max force (N) |
6747.0 (1343.3) |
6523.2 (1414.5) |
6973.6 (1678.9) |
0.7 |
|
3 PQ average peak power (W) |
1429.6 (401.2) |
1308.7 (505.2) |
1588.7 (565.6) |
0.32 |
Table note: Values are presented as mean ± SEM. No statistical significance was found in any of the physical performance tests between the vitamin D deficient, insufficient, and sufficient groups (P > 0.05).
DISCUSSION
Athletes have similar high prevalence of low 25(OH)D status as non-athletes which may negatively affect physical performance [30]. In youth athletes, 25(OH)D is necessary for bone health and muscle function which may impact physical performance. The purpose of this study was to examine the cross-sectional association between 25(OH)D status and several markers of physical performance in youth club soccer athletes. Using several different agility, muscular strength, and cardiorespiratory fitness performance markers, we found no significant associations between 25(OH)D status and any of the parameters measured between vitamin D deficient, insufficient, and sufficient groups. Interestingly, there were no performance differences between the 25(OH)D deficient and sufficient groups.
Although 25(OH)D status has been associated with muscular strength and cardiorespiratory fitness in elderly [31-34] to our knowledge, no investigation using primarily adolescent athletes has demonstrated a positive relationship between muscular strength and/or cardiorespiratory fitness. In addition, one study that supplemented youth soccer players for 8 weeks found no physical performance benefit from the vitamin D supplementation [35]. Alternatively, several investigations have shown a positive correlation between 25(OH)D status and physical performance in general population youth [26,36,37]. Ward et al., studied 12- 14 year old females with an average 25(OH)D of 21.3 nmol/L and found a positive relationship between 25(OH)D status and performance markers of jump power [26]. An investigation using Qatari adolescent girls with 25(OH)D status below 20 nmol/L, found participants with 25(OH)D levels below 10 nmol/L to have significantly lower average VO2max than those with 25(OH)D status between 10 and 20 nmol/L (mean VO2max 26.5 ± 6.3 vs. 30.7 ± 7.1 mL•kg-1•min-1, respectively). Also finding a relationship between 25(OH)D status and cardiorespiratory fitness in adolescent girls, Gracia-Marco et al., reported a positive relationship between 25(OH)D status (mean 60.2 ± 23.41 nmol/L) and VO2max (mean 36.0 ± 5.4 mL•kg-1•min-1). No relationship was found in the adolescent male population nor was there a significant relationship between 25(OH)D status and standing long jump in either of the genders [33]. Finally, Foo et al., reported adolescents who participated in sports had a statistically significant greater 25(OH)D status compared to those that did not participate in sports (mean 36.42 nmol/L vs. 30.21 nmol/L) [36]. The prior cross-sectional studies suggest a higher 25(OH)D status may be relevant to increased physical activity and higher outcomes of physical performance, specifically when 25(OH)D status is considered to be severely deficient.
Our findings do not support an association between 25(OH) D status and markers of physical performance utilizing similar performance measures as those mentioned above. Similarly, Dubnov-Raz et al. did not find an association between 25(OH)D status and balance, strength, or swim performance measures in adolescent male and female swimmers with an average 25(OH) D status of 69.14 ± 17.72 nmol/L and range between 28-135 nmol/L [24]. Orysiak et al., recruited young (average age 17 years) male hockey players with average 25(OH)D status of 75.63 ± 37.19 nmol/L and range between 31-228 nmol/L and found no correlation between 25(OH)D and muscle strength, muscle power, or anaerobic capacity [27]. Higher levels of 25(OH)D status may inhibit an association between 25(OH)D and markers of physical performance. While investigations reporting no association did include a broad range of 25(OH)D status, they enrolled a smaller percentage of vitamin D deficient participants than investigations reporting a statistically significant association.
This investigation was powered to detect small correlations and may have failed to identify the small performance differences that may occur between low and high 25(OH)D status since we only found 8 deficient participants. It should be noted that the vitamin D range in the current investigation was 39.9-104.8 nmol/L which is considerably higher than investigations finding positive associations reporting a large number of severely deficient participants [30,35]. This investigation was conducted during a single time point in the winter (January-February) and used several different measures of strength, cardiorespiratory fitness, muscular power, and agility. Therefore, we minimized the effects of seasonality on 25(OH)D status as well as seasonal changes in fitness. Additionally, we used competitive soccer athletes who are expected to perform the tests with greater skill and intensity than youth not participating in athletics. It is also possible that the training status has a greater effect on physical performance outcomes than 25(OH)D status.
CONCLUSIONS
Prior studies investigating the relationship between 25(OH) D status and physical performance have shown a positive correlation in non-athletic adolescents. The current investigation, in agreement with two others, did not find a statistically significant relationship between 25(OH)D status and physical performance in athletic adolescents. The lack of relationship may be due to higher reported range of 25(OH)D status in athletic adolescents versus the non-athletic investigations which reported a large number of severely deficient participants despite reports stating athletic populations have similar 25(OH)D status as non-athletes. Maturation and physical activity may hamper the lack of association.
AUTHOR CONTRIBUTIONS
Conceptualization, Shane Scholten and Derek Ferley; Formal analysis, Derek Ferley and Matthew Vukovich; Funding acquisition, Shane Scholten; Methodology, Shane Scholten, Derek Ferley and Matthew Vukovich; Writing – original draft, Shane Scholten and Derek Ferley; Writing – review & editing, Matthew Vukovich.
FUNDING
Research reported in this publication was supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number P20GM103443. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The results of this study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
ACKNOWLEDGMENTS
The authors would like to thank the participants for their effort, willingness, and enthusiasm for participating. They also appreciate Augustana University Exercise Science students, Clark Vargo, Alaina Klapperich, Brooke Bleeker, and Hunter Haman and staff of Avera Sports.
REFERENCES
- Christakos S, Hewison M, Gardner DG, Wagner CL, Sergeev IN, Rutten E, et al. Vitamin D: beyond bone. Ann N Acad Sci. 2013; 1287: 45-58.
- Larson-Meyer DE, Willis KS. Vitamin D and athletes. Curr Sport Med Rep. 2010; 9: 220-226.
- Larson-Meyer E. Vitamin D supplementation in athletes. Nestle Nutr Inst Workshop Ser. 2013; 75: 109-21.
- Perrone MA, Pieri M, Caminiti G, Ali W, Bernardini S, Parisi A, et al. Vitamin D Deficiency in Professional Football Players during Competitive Season of Italian First Division (Serie A). Sports. 2024; 12: 153.
- Powers S, Nelson WB, Larson-Meyer E. Antioxidant and vitamin D supplements for athletes: sense or nonsense?. J Sports Sci 29 Suppl. 2011; 1: 47-55.
- Constantini NW, Arieli R, Chodick G, Dubnov-Raz G. High prevalence of vitamin D insufficiency in athletes and dancers. Clin J Sport Med. 2010; 20: 368-371.
- Galan F, Ribas J, Sanchez-Martinez PM, Calero T, Sanchez AB, Munoz A. Serum 25-hydroxyvitamin D in early autumn to ensure vitamin D sufficiency in mid-winter in professional football players. Clin Nutr. 2012; 31: 132-136.
- Hamilton B, Grantham J, Racinais S, Chalabi H. Vitamin D deficiency is endemic in Middle Eastern sportsmen. Public Health Nutr. 2010; 13: 152834.
- Han Q, Xiang M, An N, Tan Q, Shao J, Wang Q. Effects of vitamin D3 supplementation on strength of lower and upper extremities in athletes: an updated systematic review and meta-analysis of randomized controlled trials. Front Nutr. 2024; 11: 1381301.
- Bartoszewska M, Kamboj M, Patel DR. Vitamin D, muscle function, and exercise performance. Pediatr Clin N Am. 2010; 57: 849-861.
- Close GL, Russell J, Cobley JN, Owens DJ, Wilson G, Gregson W, et al. Assessment of vitamin D concentration in non-supplemented professional athletes and healthy adults during the winter months in the UK: implications for skeletal muscle function. J Sports Sci. 2012; 22: 1–10.
- Dzik KP, Kaczor JJ. Mechanisms of vitamin D on skeletal muscle function: oxidative stress, energy metabolism and anabolic state. Eur J Appl Physiol. 2019; 119: 825-839.
- Escobedo-Monge MF, Bahillo-Curieses P, Parodi-Román J, Escobedo- Monge MA, Alonso-López P, Marugán-Miguelsanz JM. Calcium, Phosphate, and Vitamin D in Children and Adolescents with Chronic Diseases: A Cross-Sectional Study. Nutrients. 2024; 16: 1349.
- Salles J, Chanet A, Guillet C, Vaes AM, Brouwer-Brolsma EM, Rocher C, et al. Vitamin D status modulates mitochondrial oxidative capacities in skeletal muscle: role in sarcopenia. Commun Biol. 2022; 5: 1288.
- Bischoff-Ferrari HA, Giovannucci E, Willett WC, Dietrich T, Dawson-Hughes B. Estimation of optimal serum concentrations of 25-hydroxyvitamin D for multiple health outcomes. Am J Clin Nutr. 2006; 84: 18-28.
- Holick MF. The vitamin D deficiency pandemic and consequences for nonskeletal health: mechanisms of action. Mol Asp Med. 2008; 29: 361-368.
- Cannell JJ, Hollis BW. Use of vitamin D in clinical practice. Altern Med Rev. 2008; 13: 6-20.
- Zhang L, Quan M, Cao Z-B. Effect of vitamin D supplementation on upper and lower limb muscle strength and muscle power in athletes: A meta-analysis. PloS One. 2019; 14: e0215826.
- Beck KL, von Hurst PR, O’Brien WJ, Badenhorst CE. Micronutrients and athletic performance: A review. Food Chem Toxicol. 2021; 158: 112618.
- Sist M, Zou L, Galloway SDR, Rodriguez-Sanchez N. Effects of vitamin D supplementation on maximal strength and power in athletes: a systematic review and meta-analysis of randomized controlled trials. Front Nutr. 2023; 10: 1163313.
- Byers AW, Connolly G, Campbell WW. Vitamin D status and supplementation impacts on skeletal muscle function: comparisons between young athletes and older adults. Curr Opin Clin Nutr Metab Care. 2020; 23: 421.
- Dubnov-Raz G, Livne N, Raz R, Rogel D, Cohen A, Constantini N. Vitamin D concentrations and physical performance in competitive adolescent swimmers. Pediatr Exerc Sci. 2013.
- Scholten SD, Igor N Sergeev. Vitamin D and physical performance in athletes. Immun Endoc Metab Agents Med Chem. 2014; 14: 152-161.
- Ward KA, Das G, Roberts SA, Berry JL, Adams JE, Rawer R, et al. A randomized, controlled trial of vitamin D supplementation upon musculoskeletal health in postmenarchal females. J Clin Endocrinol Metab. 2010; 95: 4643–4651.
- Ferley DD, Scholten S, Vukovich MD. Combined Sprint Interval, Plyometric, and Strength Training in Adolescent Soccer Players: Effects on Measures of Speed, Strength, Power, Change of Direction, and Anaerobic Capacity. J Strength Cond Res. 2020; 34: 957-968.
- Annweiler C, Beauchet O, Berrut G, Fantino B, Bonnefoy M, Herrmann FR, et al. Is there an association between serum 25-hydroxyvitamin D concentration and muscle strength among older women? Results from baseline assessment of the EPIDOS study. J Nutr Health Aging. 2009; 13: 90-95.
- Beauchet O, Annweiler C, Verghese J, Fantino B, Herrmann FR, Allali G. Biology of gait control: vitamin D involvement. Neurology. 2011; 76: 1617-1622.
- Boxer RS, Dauser DA, Walsh SJ, Hager WD, Kenny AM. The association between vitamin D and inflammation with the 6-minute walk and frailty in patients with heart failure. J Am Geriatr Soc. 2008; 56: 454- 461.
- Dhesi JK, Jackson SH, Bearne LM, Moniz C, Hurley MV, Swift CG, et al. Vitamin D supplementation improves neuromuscular function in older people who fall. Age Ageing. 2004; 33: 589-595.
- Skalska M, Nikolaidis PT, Knechtle B, Rosemann TJ, Radzimi?ski ?, Jastrz?bska J, et al. Vitamin D Supplementation and Physical Activity of Young Soccer Players during High-Intensity Training. Nutrients. 2019; 11: 349.
- Foo LH, Zhang Q, Zhu K, Ma G, Trube A, Greenfield H, et al. Relationship between vitamin D status, body composition and physical exercise of adolescent girls in Beijing. Osteoporos Int. 2009; 20: 417-425.
- Gilic B, Kosor J, Jimenez-Pavon D, Markic J, Karin Z, Domic DS, et al. Associations of Vitamin D Levels with Physical Fitness and Motor Performance; A Cross-Sectional Study in Youth Soccer Players from Southern Croatia. Biology. 2021; 10: 751.
- Angeline ME, Gee AO, Shindle M, Warren RF, Rodeo SA. The effects of vitamin D deficiency in athletes. Am J Sports Med. 2013; 41: 461-464.
- Gracia-Marco L, Valtuena J Fau - Ortega FB, Ortega Fb Fau - Perez- Lopez FR, Perez-Lopez Fr Fau - VRG, Vicente RG Fau - Breidenassel C, Breidenassel C Fau - Ferrari M, et al. Iron and vitamin status biomarkers and its association with physical fitness in adolescents: the HELENA study. J Appl Physiol. 2012; 113: 566-573.
- Orysiak J, Mazur-Rozycka J, Fitzgerald J, Starczewski M, Malczewska- Lenczowska J, Busko KA-O. Vitamin D status and its relation to exercise performance and iron status in young ice hockey players. PLoS One. 2018; 13: e0195284.
- Racinais S Fau - Hamilton B, Hamilton B Fau - Li CK, Li Ck Fau - Grantham J, Grantham J. Vitamin D and physical fitness in Qatari girls. Arch Child. 2010; 95: 854-855.
- Ward KA, Das G, Berry JL, Roberts SA, Rawer R, Adams JE, et al. Vitamin D status and muscle function in post-menarchal adolescent girls. J Clin Endocrinol Metab. 2009; 94: 559-563.








































































































































