Two Week Keratin-Based Protein Supplementation is Comparable in Gastrointestinal Handling to a Milk-Based Equivalent
- 1. School of Sport and Exercise, Massey University, New Zealand
Abstract
Purpose: Keratins are fibrous, structural, animal-based proteins with emerging potential as a supplement for humans. Naturally high levels of the sulfur amino-acid cysteine suggest that keratin ingestion could augment antioxidant status and provide benefit for healthy and diseased populations. Although keratins have long been present in the human diet, scientific confirmation of gastrointestinal and metabolic acceptability during daily keratin intake representing a significant proportion of daily minimum recommended protein intake is required.
Methods: In a blind cross-over study, questionnaire based assessment of gastrointestinal health and palatability was undertaken every 3 days during 14 days of daily consumption of either casein or a keratin based bar and drink powder. Ingestion rate began at 10 g?d-1 of target protein and increased by 10 g every 3 days ending with 5 days at 40 g?d-1.
Results: Keratin ingestion raised the prevalence of increased flatulence and change in flatulent odor compared to the casein control. No other negative trends in gastrointestinal health or dose response were observed within or between the two treatments.
Conclusions: The keratin-based protein supplementation up to 40 g?d-1 for 5 days did not cause any acute gastrointestinal disturbance unrelated to the consumption of high-protein supplements. This finding creates the opportunity for further research relating to the proposed health and/or ergogenic benefits of keratin protein ingestion for athletes and the general population.
Keywords
• Keratin
• Protein
• Supplement
• Antioxidants
• Cysteine
Citation
Houltham S, Starck C, Stannard S (2014) Two Week Keratin-Based Protein Supplementation is Comparable in Gastrointestinal Handling to a Milk-Based Equivalent. J Hum Nutr Food Sci 2(4): 1040.
INTRODUCTION
Keratins are a family of fibrous structural proteins that provide functional rigidity to a large number of animal tissues. They have long been present in the human diet; normally eaten in conjunction with animal food sources, such as when skin and hair are consumed. Certainly, keratin proteins ingested in this manner contribute only small proportions of total protein intake, and their bioavailability may be much lower than other proteins. Larger quantities of keratin are present within animal tissues with rigid protein matrices such as feathers and wool. Isolation of keratins from these tissues yields a digestible raw protein product with potentially significant nutritional value. The naturally high levels of the amino acid cysteine in keratin suggest potential for dietary enhancement of the biological thiols taurine and glutathione, which have diverse and important roles in health including potent antioxidant activity [1,2]. Furthermore, keratins are a source of mixed amino acids which may have broad application as a protein supplement. Processing of animal tissues into a raw keratin product would allow levels of consumption that vastly exceed those from traditional sources. Therefore, robust testing of keratin protein ingestion in quantities that represents a substantial proportion of typical daily protein intake is warranted.
In the laboratory, keratins are shown to have naturally very poor digestibility by trypsin and pepsin. While the high cysteine content of keratin has significant nutritional potential, it also contributes to enhanced structural rigidity. The sulfurcontaining side chains of cysteine form highly stable disulfide bonds that are resistant to heat and digestive enzymes. Although recent techniques have been developed to process a highly digestible keratin protein hydrosylate from feather meal for the production of animal feed [3], hydrolytic methods can produce a large proportion of peptides that tend to be bitter. A novel proprietary method that isolates keratin from poultry feathers using minimal hydrolysis has been proposed to create a more digestible and palatable product for human consumption (Keraplast Technologies).
Ingestion of keratin-protein may enhance antioxidant status, exercise performance, and health by delivering a precursor of the diverse bio-regulatory thiol; taurine and the antioxidant glutathione (GSH). High dietary levels of sulfur amino-acids have been shown to directly stimulate taurine biosynthesis [2]. Animal studies show taurine can inhibit oxidative damage to DNA at normal cellular concentrations [4] and reduce superoxide radical production in rat muscle following eccentric exercise [1]. Evidence in humans is scarce, yet, taurine supplementation in young men showed a moderate association between the level of taurine supplementation, exercise performance and the presence of the lipid peroxidation marker; TBARS [5].
Cysteine ingested in the form of N-acetylcysteine (NAC) directly increases intracellular glutathione levels and up-regulates its antioxidant activity [6,7]. NAC supplementation has also been shown to improve muscle function during prolonged submaximal cycling [8], and increase Erythropoietin and Hemoglobin levels in healthy men [7, 9]. However, high levels of supplementation with antioxidants or their precursors could potentially disrupt other redox-sensitive signaling pathways involved in cellular repair and adaptation [10]. An NAC-mediated increase in GSH has been shown to disrupt the skeletal muscle inflammatory response and repair capability in recreationally-trained men performing muscle-damaging exercise[11]. Therefore the exact benefits of dietary cysteine ingestion with respect to increasing GSH biosynthesis remain controversial.
A caveat of the production process used for the investigated keratin protein product is the 97% conversion of cysteine to cysteic acid. Cysteic acid cannot be incorporated into GSH but is a direct precursor to taurine [12]. Taurine supplementation has been shown to increase GSH levels in rats [13] likely by increasing the availability of cysteine and methionine for GSH production. Also, most keratins contain only low concentrations of several essential amino acids (histidine, lysine, and tryptophan), which suggests the overall quality of Keratin protein is lower than other protein sources.
Keratin proteins are novel as both a major contributor to dietary protein and a potential source of antioxidants, therefore, verification of their daily consumption at doses equivalent to other dietary protein sources is needed as a prelude to further investigation of their therapeutic and ergogenic potential. The described keratinous protein-based food supplement is proposed to be both digestible and palatable. In this study, we utilized a blinded, randomized, cross-over design to compare the effect of daily keratin protein ingestion for two weeks on gastrointestinal perceptions relative to a milk-derived (casein) equivalent.
MATERIALS AND METHODS
Participants
Seventeen males aged on average (SD) 30 (9.4) years, standing 182 (7.6) cm tall and weighing 79 (7.0) kg participated in the study. Inclusion criteria required participants to have exercised a minimum of 3 hours per week in the previous 6 months and have a BMI of less than 27. All participants received verbal and written descriptions from the researchers detailing the purpose of the study, rights, requirements, and associated risks; participants were screened for precluding health conditions and gave written consent to participate. The study was approved by the Massey University Human Ethics Committee (Southern A, application 13/04).
Study design
The study was a blind, randomized, cross-over design consisting of two 14-day blocks interspersed with a 2-week washout period. In each block, participants were supplied with daily portions of drink powder and a bar delivering equal amounts of the target protein. A ramped dose protocol was used to allow for monitoring of side effects related to increased keratin ingestion. The dose of target protein began with 10 g?d-1 for 3 days followed by 3 days at 20 g?d-1, 3 days at 30 g?d-1 and 5 days at 40 g?d-1. Supplements could be consumed at any time of the day and participants were asked to consume the bar and drink a minimum of 2 hours apart. Participants were instructed to remove snack items from their background diet to make way for the supplements, and were advised to maintain their dietary intake and routine relative to the normal dietary cues of satiety and meal timing.
Supplements
The keratin protein was manufactured by Keraplast Technologies Ltd. using a proprietary method under the trade name Kerapro. A commercially available casein protein was used for the control condition.The typical amino acid profiles of the keratin and casein proteins are illustrated in (Table 1).
Table 1: Representative amino acid profiles of keratin and casein proteins.
| Amino Acid | Grams of anhydrous amino acid per 100 grams of protein | |
| Keratin | Casein | |
| Alanine | 4.2 | 2.7 |
| Arginine | 7.0 | 3.7 |
| Aspartic Acid | 7.6 | 6.9 |
| Cysteine Cysteic Acid |
0.35 6.15 |
0.3 - |
| Glutamic Acid | 11.8 | 23.2 |
| Glycine | 6.3 | 2.4 |
| Histidine | 0.5 | 2.8 |
| Isoleucine | 5.3 | 5.5 |
| Leucine | 8.3 | 9.2 |
| Lysine | 1.2 | 7.4 |
| Methionine | 0.4 | 2.5 |
| Phenylalanine | 4.6 | 4.9 |
| Proline | 10.0 | 10.7 |
| Serine | 10.6 | 4.4 |
| Threonine | 4.9 | 1.1 |
| Tryptophan | - | 1.2 |
| Tyrosine | 2.1 | 5.7 |
| Valine | 8.8 | 6.5 |
On average, 94.6% of the cysteine in keratin is present as cysteic acid due to the minimal hydrolysis used in protein isolate production. Amino acid analysis was performed by the Nutrition Laboratory at Massey University, Palmerston North, as well as the Australian Proteome Analysis Facility (APAF http://www.proteome.org.au) with consistent results.
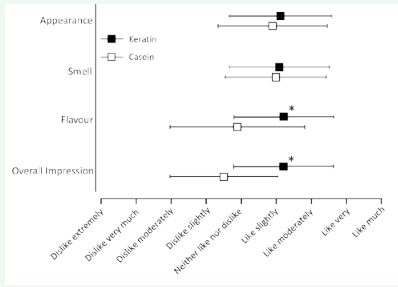
Figure 1: Comparison of sensory impressions of keratin and casein protein bars.
*denotes significant difference between conditions (p = <0.05)
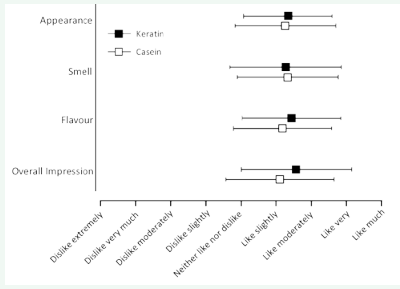
Figure 2: Comparison of sensory impressions of keratin and casein protein drinks.
Drink powder: The drink powder contained ~67% per unit weight of the target protein. Carbohydrate and fat content were ~ 19% and 4% respectively. Non-target protein content was ~2% coming from cocoa. Two flavors of drink powder were used in the study (chocolate orange and chocolate mint). Participants were supplied with a specified mixing container and asked to mix the powder with water or milk. The first dose contained 7.5 grams of powder which was to be mixed with 150 ml of fluid.
Bar: Each bar contained ~34% of the target protein per unit weight. Carbohydrate content was ~45% and fat content was ~8%. Non-target protein content was ~1.3% coming from cocoa. Two flavors of bar were used in the study (chocolate and banana). The entire surface of the bars was coated in a thin (~2mm) layer of chocolate.
Questionnaires
Gastrointestinal health was monitored using a “health/side effects” questionnaire. The questionnaire asked participants whether they were experiencing heartburn, nausea, loss of appetite, belching, borborygmi (stomach rumbling), indigestion, colic, or a change in their stool, flatulence, energy levels, sleeping patterns, mood, or pre-existing medical conditions during the previous 3 days of supplementation.
Palatability of the bar and drink was assessed separately using a 9-point scale consumer hedonics questionnaire. Participants were asked to rank the appearance, smell, flavor and overall impression of the bar and drink on a 9-point scale from “dislike extremely” to “like much”. Each question contained a voluntary comments field for qualitative feedback.
Procedures
Prior to each supplementation block, participants were supplied with 14 days of pre-packaged daily amounts of either the casein or keratin based drink and bar. Gastrointestinal health and palatability questionnaires were completed on days 3, 6, 9, and 14 of each block. Following a ~2-week washout period, the protocol was repeated using the alternate protein source.
Analysis
The 9-point subjective scale used to assess palatability was converted to a numerical 1 – 9 scale. Mean and standard deviations were then calculated for the data. The gastrointestinal health data was tallied by the occurrence of either yes or no, then displayed in table form. Chi-squared statistical analysis was used to determine significance between conditions.
Results
All 17 participants who began the study completed the crossover protocol. No participants suffered from undue pain or discomfort relating to either protein source or to the inclusion of protein supplements per se into the diet.
Gastrointestinal health
Overall, there was a tendency for more symptoms to appear during the keratin (81) treatment than the casein (34). Of the symptoms measured, approximately half of this variance can be attributed to the increase in flatulence (K: 26, C: 3) alone.
Severity of symptoms
No participants withdrew during the study due to adverse gastrointestinal disturbances or other illnesses. Overall, only one case of moderate GI upset was reported. This occurred on day 9 of the keratin block, but symptoms subsided throughout the remainder of the block. A further three participants experienced slight queasiness (2 on day 9, 1 on day 14). All cases of nausea were accompanied by borborygmi. On 4 other occasions, borborygmus was experienced without nausea. 12 of the 17 participant did not experience any borborygmi or nausea symptoms at any time during keratin ingestion.
Flatulence
Overall, 13 of the 17 participants experienced an increase in the amount and a change in odor of their flatulence at some stage during keratin supplementation. The occurrence of flatulence increased slightly with each increase in daily dose (Table 2); however, a dose response relationship was not evident. Four participants did not observe changes in flatulence across the 14 day keratin block and only 2 participants reported a persistent change across the 14 days. Two participants reported a subsidence in flatulence after 3 days.
Table 2: Overview of symptoms during 14 day keratin and casein supplementation.
| Symptoms | Keratin | Casein | |||
| Yes | No | Yes | No | ||
| 1 | Did you experience heartburn | 3 | 65 | 3 | 65 |
| 2 | Did you experience nausea/vomiting | 5 | 63 | 2 | 66 |
| 3 | Lost appetite | 4 | 64 | 1 | 67 |
| 4 | Did you experience belching | 0 | 68 | 3 | 65 |
| 5 | Did you experience borborygmi | 9 | 59 | 2 | 66 |
| 6 | Did you suffer from Indigestion | 2 | 66 | 1 | 67 |
| 7 | Did you suffer from colic | 1 | 67 | 1 | 67 |
| 8 | Did you experience a change in frequency or consistency of your stools | 13 | 55 | 7 | 61 |
| 9 | Did you experience noticeable change in amount or odor of flatulence | 26* | 42 | 3 | 665 |
| 10 | Did you feel changes in energy levels | 8 | 60 | 5 | 63 |
| 11 | Did you notice obvious changes in sleeping patterns | 3 | 65 | 0 | 68 |
| 12 | Did you notice any changes in your mood | 2 | 66 | 0 | 68 |
| 13 | Did your weight change noticeably | 1 | 67 | 0 | 68 |
| 14 | Did you notice any marked changes in pre-existing medical conditions | 0 | 68 | 1 | 67 |
| 15 | Did you notice any marked changes in appetite | 5 | 63 | 5 | 63 |
| Total | 81 | 939 | 34 | 986 | |
*denotes significant difference between conditions (p = <0.05).
Table 3. Summary of symptom prevalence at each dose during the keratin and casein blocks.
| Symptoms | Keratin | Casein | |||||||||||||||
| Day 3 | Day 6 | Day 9 | Day 14 | Day 3 | Day 6 | Day 9 | Day 14 | ||||||||||
| Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | ||
| 1 | Heartburn | 1 | 16 | 2 | 15 | 0 | 17 | 0 | 17 | 1 | 16 | 0 | 17 | 0 | 17 | 2 | 15 |
| 2 | Nausea/vomiting | 1 | 16 | 1 | 16 | 2 | 15 | 1 | 16 | 1 | 17 | 1 | 16 | 0 | 17 | 1 | 16 |
| 3 | Lost appetite | 0 | 17 | 1 | 16 | 2 | 15 | 1 | 16 | 0 | 17 | 0 | 17 | 0 | 17 | 1 | 16 |
| 4 | Belching | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 1 | 16 | 1 | 16 | 0 | 17 | 1 | 16 |
| 5 | Borborygmi | 3 | 15 | 1 | 16 | 2 | 15 | 3 | 14 | 0 | 17 | 0 | 17 | 1 | 16 | 0 | 17 |
| 6 | Indigestion | 1 | 16 | 0 | 17 | 0 | 17 | 1 | 16 | 0 | 17 | 1 | 16 | 0 | 17 | 0 | 17 |
| 7 | Colic | 0 | 17 | 1 | 16 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 1 | 16 |
| 8 | Consistency of stool | 2 | 15 | 2 | 15 | 3 | 14 | 6 | 11 | 1 | 16 | 2 | 15 | 0 | 17 | 4 | 13 |
| 9 | Flatulence | 4 | 13 | 5 | 12 | 7* | 10 | 10* | 7 | 1 | 16 | 2 | 15 | 0 | 17 | 0 | 17 |
| 10 | Energy | 4 | 13 | 2 | 15 | 0 | 17 | 2 | 15 | 2 | 15 | 1 | 16 | 1 | 16 | 1 | 16 |
| 11 | Sleeping patterns | 1 | 16 | 0 | 17 | 1 | 16 | 1 | 16 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 |
| 12 | Mood | 1 | 16 | 1 | 16 | 0 | 16 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 |
| 13 | Weight | 0 | 17 | 0 | 17 | 1 | 16 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 |
| 14 | Change in pre-existing medical conditions | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 0 | 17 | 1 | 16 |
| 15 | Change in appetite | 0 | 17 | 1 | 16 | 2 | 15 | 2 | 15 | 1 | 16 | 0 | 17 | 2 | 15 | 2 | 15 |
| Total | 18 | 239 | 17 | 239 | 20* | 236 | 27* | 229 | 7 | 249 | 8 | 248 | 4 | 252 | 14 | 242 | |
*denotes significant difference between conditions (p = <0.05)
PALATABILITY
There were no significant differences in the palatability of the casein and keratin drink. The keratin bar was perceived to be better overall compared to the casein bar. These results may have reflected the challenge in creating bars that matched in texture and flavor. Nevertheless, the participants were blinded to the treatment order and therefore a relationship between palatability and GI handling is unlikely and not evident from the data.
DISCUSSION
The main finding of this study was that daily consumption of keratin protein up to 40 g?d-1 for five days did not cause major adverse gastrointestinal distress or result in other acute-onset health consequences. Of the responses monitored, a general increase and change in odor of flatulence with keratin consumption was the only statistically more prevalent gastrointestinal response compared to casein ingestion. To our knowledge, these findings provide the first evidence within a controlled setting that daily consumption of keratin-derived protein sources is safe up to levels approximately half recommended minimum daily protein requirement of 0.8 g?kg-1?d-1.
The change in flatulence during the keratin treatment was an anticipated response to cysteine-rich and therefore sulfurrich protein. The concentration of sulfur compounds in flatus is likely to be dose-dependent with sulfur amino-acid intake [14]. Fermentation of ingested protein in the GI tract releases sulfur gases and only very small amounts are needed to be detectable by smell. Despite the unpleasant nature of increased flatulence, only one participant reported moderate gastrointestinal upset in conjunction with a change in flatulence, with a further 12 participants reporting flatulence but no other GI distress. Furthermore, despite the higher incidence of flatulence with increase daily dose, 7 of the 17 participants did not report flatulence at the highest dose, and 3 participants reported a subsidence in flatulence throughout the 14-day keratin block. Our findings do show a weak association between dose and increased flatulence, however since no association could be made with any other GI responses, the increase in flatulence is not a candidate for precluding keratin as a food source.
We cannot be certain whether the gastrointestinal disturbances observed were caused by keratin or by high levels of dietary protein. Mild gastrointestinal disturbance is common in the first few days of daily protein supplementation. Analysis showed that borborygmi was more prevalent in the first block regardless of the protein source (keratin: 7, casein: 6). A dose response was not observed indicating that keratin proteins can be consumed safely up to ~40 g?d-1.
Our palatability data showed that the perception of the taste and texture of the supplements tended to remain the same or in fact enhance throughout the two week blocks. No participant reached a stage where they could not continue consuming the products due to no longer being able to tolerate the taste or texture of the keratin or casein supplements, even as the daily quantity increased. Several participants noted that the largest protein dose became difficult to consume due to the quantity of food rather than due to taste or texture. No relationship could be found between the appearance of gastrointestinal symptoms and taste perception. Many participants who indicated a change in stool, or a change in the odor of flatulence tended to enjoy daily consumption of the supplements.
CONCLUSION
To our knowledge this study is the first to assess the effects of daily keratin consumption at doses above one gram and up to a significant proportion of daily protein requirement. Our data show that the keratin supplements consumed up to 40 g?d-1 for 5 days did not cause adverse gastrointestinal or other acute onset illness, and is therefore safe for general consumption. Further work is needed to determine the effect of keratin ingestion on biochemical pathways involving thiol and antioxidant regulation. The current study provides a basis for future investigations which will determine the efficacy and effectiveness of keratin protein as a nutritional supplement for diseased and healthy populations.
CONFLICT OF INTEREST
1This project was funded by Keraplast Technologies Ltd, Christchurch, NZ
Author disclosure: no conflicts of interest.
REFERENCES
12. Osman, L.P., S.C. Mitchell, and R.H. Waring, Cysteine, its Metabolism and Toxicity. Sulfur reports, 1997. 20(2): p. 155-172.








































































































































